Beyond the Surface: A Clinical Comparison of DEEP OSCILLATION® and Modern Therapeutic Modalities
This article explains DEEP OSCILLATION®, a non-invasive medical technology that uses electrostatic impulses to treat a variety of clinical conditions. Unlike traditional heat-based therapies, this method is athermic, making it exceptionally safe for patients with metal implants, acute injuries, or severe swelling. The technology penetrates up to 8 cm deep into tissue layers, effectively promoting lymphatic drainage, reducing inflammation, and accelerating wound and scar healing. Because it requires no physical downward pressure, it offers ergonomic benefits for practitioners while remaining gentle enough for sensitive populations such as infants and the elderly. The article also highlights the device's versatility across fields such as sports medicine, post-surgical recovery, and chronic condition management, providing a clear comparison against other modern therapeutic modalities.

Table of Contents
- Introduction and Keywords
- Mechanism and Depth of Action
- Safety and Versatility Over Metal and Oedema
- Comparisons with Negative Pressure Therapy
- Comparisons with Radiofrequency Diathermy
- Comparisons with Extracorporeal Shockwave Therapy (ESWT)
- Comparisons with Laser Therapy (LLLT)
- Clinical Application and Therapist Ergonomics
- Continuity of Care: At-Home Treatment and Patient Self-Care
- Modality Comparison Matrix
- Clinically Proven Physiological Effects
- Conclusion
- Glossary of Clinical Terms
- AI Disclosure Statement
- References
- Suggested Citation and Sharing Policy
List of Figures
Figure 1. A 3D anatomical cross-section of the 8cm depth of deep oscillation
Figure 2. Application of deep oscillation
Figure 3. Comparison of modern therapeutic modalities
Figure 4. Clinically proven effects of deep oscillation
1. Introduction
As the clinical landscape of physical therapy advances, practitioners are equipped with an increasingly diverse array of high-tech modalities. However, in today’s challenging economic climate, clinics and independent therapists are increasingly mindful of their capital investments. Rather than purchasing multiple single-indication devices, practitioners are actively seeking versatile, "all-rounder" equipment capable of safely treating a broad spectrum of patient presentations. Because it is completely non-invasive and a-thermic, DEEP OSCILLATION® can be safely applied to almost any demographic—from babies and the elderly to elite athletes, and even complex post-surgical patients with passive metal implants.
Because DEEP OSCILLATION® offers exactly this level of clinical adaptability, a recurring question we frequently receive is: How exactly does it differ from other therapies on the market? This article aims to provide a clear, evidence-based comparison to help practitioners understand exactly where deep oscillation fits within the broader landscape of physical rehabilitation and tissue healing.
Keywords: DEEP OSCILLATION®, Electrotherapy, Radiofrequency Diathermy, Negative Pressure Massage, Oedema Management, Tissue Resonance, A-thermic Modalities, Self-Treatment, LLLT, Shockwave Therapy.
2. Mechanism and Depth of Action
The fundamental difference between deep oscillation and conventional electrotherapies lies in how they interact with the body. While conventional electrotherapies, such as TENS, act primarily on the neuromuscular system (Burgess et al., 2019), deep oscillation acts within the interstitial spaces of the connective tissue.
By utilising the Johnsen-Rahbek effect, it permeates deeply into the tissue—a resonant vibration effect initially confirmed by diagnostic ultrasound to a depth of 8 cm (Hernández Tápanes, 2010), and subsequently verified in a large-scale clinical trial involving 401 participants (Hernández Tápanes et al., 2018). This 8 cm depth of action, which gently affects the skin, connective tissue, subcutaneous fat, muscles, and blood and lymphatic vessels, is visually represented in the anatomical cross-section below (Figure 1).
Furthermore, unlike ultrasound, radiofrequency diathermy, or shortwave therapies, deep oscillation does not produce any endogenous heat, is not magnetic, and has no electromagnetic field (Jahr, Schoppe and Reisshauer, 2008; Vladeva, Mihaylova and Panayotova, 2021). This unique a-thermic profile allows it to be used safely in acute situations where other therapies are strictly contraindicated.
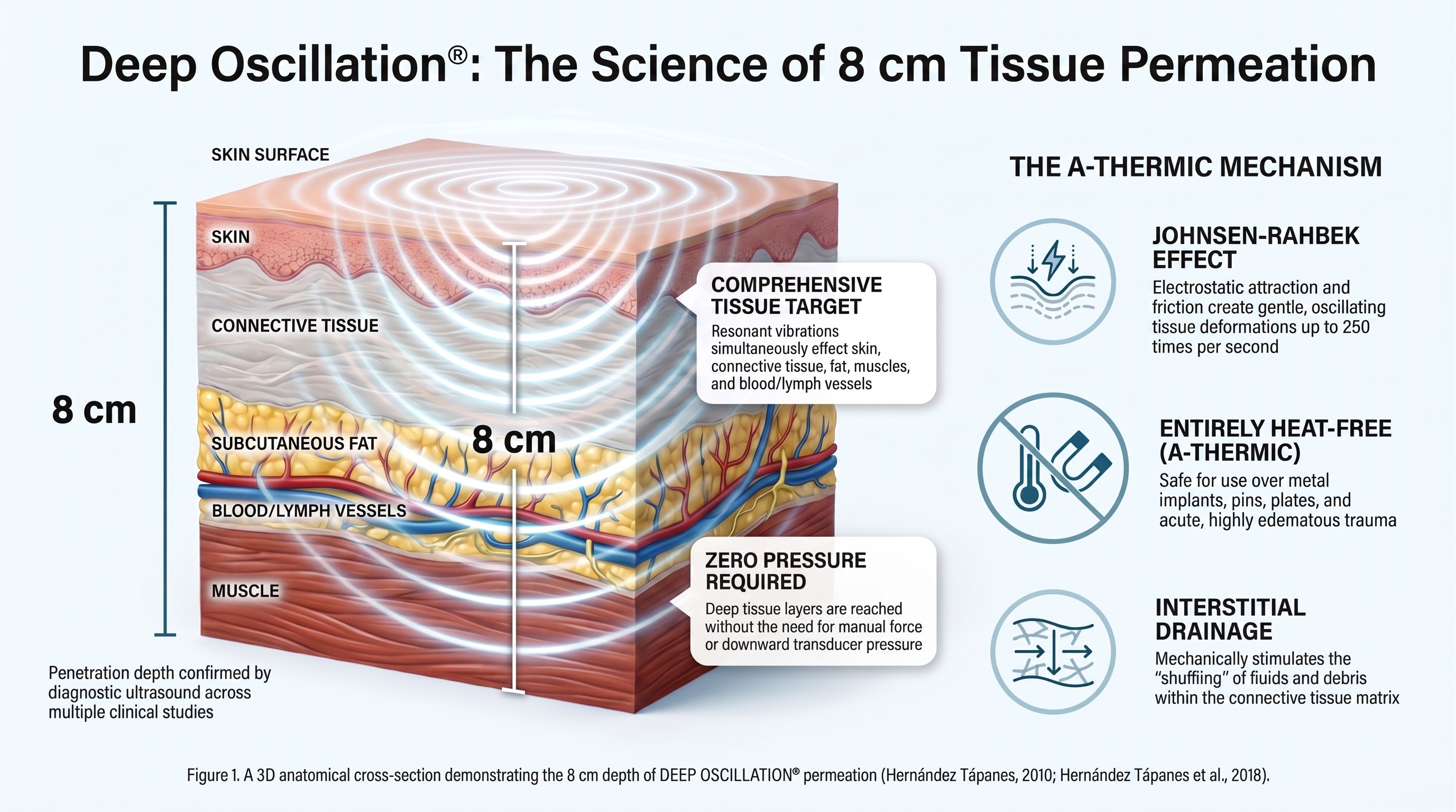
Figure 1. A 3D anatomical cross-section demonstrating the 8 cm depth of DEEP OSCILLATION® permeation (Hernández Tápanes, 2010; Hernández Tápanes et al., 2018).
3. Safety and Versatility Over Metal and Oedema
Modalities that generate deep endogenous heat, such as ultrasound and radiofrequency diathermy, are widely contraindicated over metal, cement, or plastic implants due to the severe risk of internal thermal build-up (Ferriero et al., 2020; Lupowitz et al., 2025). Conversely, athermic (heat-free) modalities are generally safe to use over passive metal implants such as pins and plates. Recent clinical evidence confirms that passive metal implants do not contraindicate electrical stimulation when applied at therapeutic intensities, as the electrical current does not cause harmful heating (Sinclair et al., 2023; Thaler, Toledo and Korte, 2017).
Furthermore, because deep oscillation is entirely a-thermic, it is completely safe to use over breast implants and prostheses without causing thermal damage (Hernández Tápanes et al., 2018; Jahr, Schoppe and Reisshauer, 2008).
Deep oscillation also stands alone in its ability to safely treat acutely swollen, heavily swollen tissues. While conventional electrotherapies like TENS face moderate clinical precautions when applied over extreme oedema, as excess fluid can adversely affect current conduction and patient comfort (Burgess et al., 2019), deep oscillation acts gently within the interstitial spaces. Because it permeates deeply using intermittent electrostatic impulses with a minimal external mechanical effect, it is uniquely safe and effective in acute, highly oedematous trauma situations (Vladeva, Mihaylova and Panayotova, 2021).
4. Comparisons with Negative Pressure Therapy
While both deep oscillation and negative pressure therapy are excellent for lymphatic drainage, oedema management, and scar tissue, they achieve these benefits through entirely different mechanisms. Negative pressure therapy uses mechanical suction and high-frequency vibration to physically pull, expand, and stretch the skin and fascial structures (Iivarinen, Korhonen and Jurvelin, 2013). In contrast, deep oscillation uses intermittent electrostatic impulses to create attraction and friction, lifting and dropping the tissue without requiring any physical pressure or suction (Vladeva, Mihaylova and Panayotova, 2021). Both modalities are safe to use over orthopaedic metalwork and titanium implants, as evidenced by clinical rehabilitation studies involving post-operative trauma patients (Dresing et al., 2021; Vladeva, Mihaylova and Panayotova, 2021).
5. Comparisons with Radiofrequency Diathermy
Radiofrequency diathermy (clinically known as Capacitive and Resistive Electric Transfer or CRET) uses high-frequency radiofrequency current to generate endogenous heat and target deeper tissues, such as bones and tendons, specifically when used in Resistive (RET) mode (Fatu et al., 2025; Lupowitz et al., 2025). Because this form of diathermy relies on thermal energy transfer, it is generally contraindicated over metal, cement, or plastic implants due to deep thermal risks (Ferriero et al., 2020). Conversely, deep oscillation utilises entirely a-thermic (heat-free) intermittent electrostatic impulses, ensuring it can be applied safely over orthopaedic materials without any thermal risk (Jahr, Schoppe and Reisshauer, 2008).
6. Comparisons with Extracorporeal Shockwave Therapy (ESWT)
Extracorporeal Shockwave Therapy (ESWT) utilises high-energy acoustic waves to treat musculoskeletal disorders, and has been shown to be effective in managing conditions such as lipoedema by breaking down fibrotic and calcified tissues (Bruno and Cilluffo, 2025; Durmu? et al., 2025). However, because it relies on high-energy acoustic force, ESWT is generally contraindicated directly over metal implants and pins, and can be painful for patients with hypersensitive superficial tissues. In contrast, deep oscillation achieves fibrosis reduction and tissue mobilisation through gentle, pain-free electrostatic attraction and friction, making it suitable for highly sensitive or acute presentations.
Notably, recent clinical trials demonstrate that these two modalities work exceptionally well in synergy.
A 2024 experimental study in the Journal of Aesthetic Nursing evaluated the combined use of shockwave therapy and deep oscillation on patients with lipoedema. The researchers concluded that the combination of both modalities promoted a superior reduction in limb perimetry, a lower percentage of fat, and a significantly greater visual and qualitative improvement in the lipoedema tissue compared to using either therapy in isolation (Almendras et al., 2024).
7. Comparisons with Laser Therapy (LLLT)
Low-Level Laser Therapy (LLLT) operates on the principle of photobiomodulation, utilising light energy to penetrate the tissue, reduce inflammation, and promote superficial tissue healing (Fatu et al., 2025). Because LLLT does not rely on deep endogenous heat or physical force, it is generally considered safe for use over metal implants. However, its photobiomodulation is typically limited to penetrating only a few centimetres, whereas deep oscillation safely permeates up to 8 cm.
Furthermore, because laser relies on light absorption rather than physical tissue manipulation, it does not provide the mechanical "lifting and dropping" effect required to actively relax severe muscle spasms or physically pump lymphatic fluid.
8. Clinical Application and Therapist Ergonomics
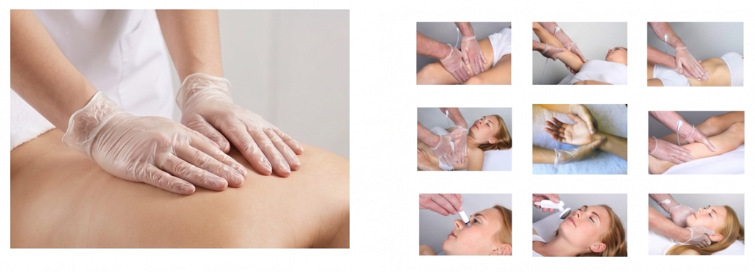
Figure 2. Clinical application of DEEP OSCILLATION® utilising the gloved-hand method or applicator/s across various anatomical regions.
-
One of the most significant practical distinctions between these modalities lies in the method of application and its resulting ergonomic impact on the practitioner. In practice, deep oscillation is uniquely applied directly through the therapist's gloved hands or handheld applicators (Figure 2). Because this mechanism does not require any physical downward pressure to reach deep tissue layers, it significantly protects the practitioner's hands and wrists from repetitive strain and fatigue while preserving essential tactile sensitivity.
Universal Application and Therapist Safety:
- Patients of All Ages (From Babies to the Elderly): Because it operates via intermittent electrostatic impulses rather than mechanical force, the therapy does not require any physical downward pressure to reach deep tissue layers. This makes it exceptionally gentle, non-traumatic, and completely safe for fragile demographics like infants and older adults (Medina, 2017).
- Complex Post-Surgical Patients: Unlike deep-heating modalities, deep oscillation produces no endogenous heat and has no electromagnetic field. This purely a-thermic profile means it is completely safe to apply directly over passive metal implants, pins, plates, and breast prostheses without any risk of thermal tissue damage (Hernández Tápanes et al., 2018; Jahr, Schoppe and Reisshauer, 2008).
- Acute Trauma Patients: Because the therapy acts gently within the interstitial spaces with minimal external mechanical force, it is uniquely safe and effective to use on acute, heavily swollen, and highly oedematous trauma presentations where traditional massage is often contraindicated. It can even be applied in the extremely early stages, such as day one post-surgery (Vladeva, Mihaylova and Panayotova, 2021).
- Elite Athletes and Sports Professionals: The deep, resonant vibrations actively enhance lymphatic drainage, clear metabolic waste, and relieve severe muscle spasms. This rapid reduction in pain and swelling accelerates recovery from muscle microtrauma (DOMS) and allows athletes to return to weight-bearing rehabilitation much sooner (von Stengel et al., 2018).
- Therapist Safety: The technology features a patented active discharge system, meaning the field disintegrates during each interval as the polarity changes, so the therapist does not store an electrostatic charge. Clinical studies show no statistically significant changes in a therapist's microcirculation, blood pressure, or heart rate after applying the therapy (Portnov and Zabelina, 2002).
9. Continuity of Care: At-Home Treatment and Patient Self-Care
The ability to continue rehabilitation between clinical appointments is a crucial factor in optimising patient outcomes. Conventional electrotherapies, such as TENS, are widely recognised and accessible for at-home neuromuscular pain relief (Burgess et al., 2019). Similarly, Low-Level Laser Therapy (LLLT) devices can be safely operated by patients at home for superficial tissue treatment and to reduce inflammation (Fatu et al., 2025).
For deep tissue, lymphatic, and post-surgical care, deep oscillation offers dedicated "Personal" units (Basic and Pro). These portable devices feature pre-programmed indication lists, allowing patients to safely self-treat with handheld applicators to maintain clinical results between appointments. Partners and supportive others (contraindications checked) can also apply to the patient using the gloved-hand method.
While some negative pressure therapy devices are also intended for at-home users, they are officially classified as prescription-only (Rx) medical devices. Because they utilise active mechanical suction, any at-home user must be knowledgeable and properly trained under the direct supervision of a healthcare professional (Iivarinen, Korhonen and Jurvelin, 2013). Conversely, deep-heating modalities such as ultrasound and radiofrequency diathermy remain strictly in-clinic, professional-only tools due to the complexities of application and the risks associated with deep endogenous heat (Lupowitz et al., 2025).
10. Modality Comparison Matrix
The following clinical comparison matrix outlines the primary mechanisms, target areas, and safety profiles of modern therapeutic modalities (Figure 3). Notably, deep oscillation is uniquely distinguished by its use of a-thermic, intermittent electrostatic impulses that safely permeate all tissue layers to a depth of 8 cm without requiring physical downward pressure. This mechanism ensures it is entirely safe for application over passive metal implants, prostheses, and acute oedema, whereas high-energy and deep-heating modalities (such as shockwave, radiofrequency diathermy, and ultrasound) are generally contraindicated in these sensitive environments. Furthermore, the therapy remains highly effective in treating long-term chronic conditions, offering a complete continuum of care.
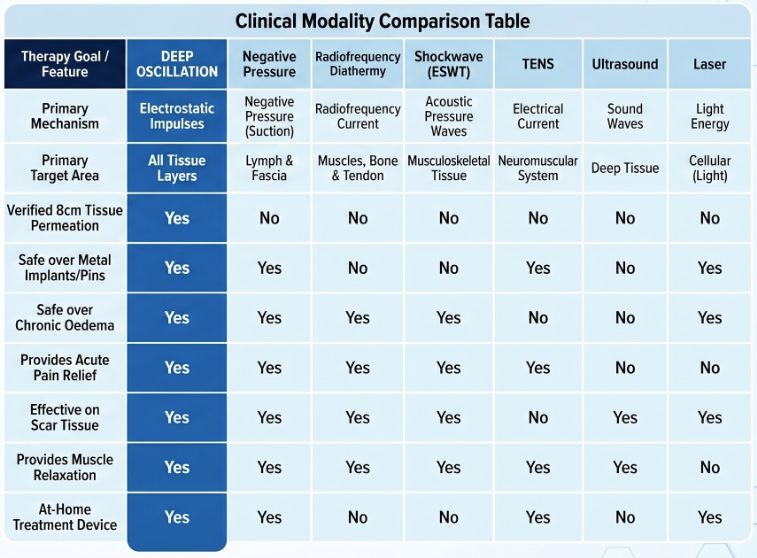
Figure 3. Comparison of modern therapeutic modalities
* Clinical Note: The information presented in this comparison matrix is based on scientifically verified data, diagnostic ultrasound findings, and peer-reviewed clinical studies, as detailed in the reference list of this article.
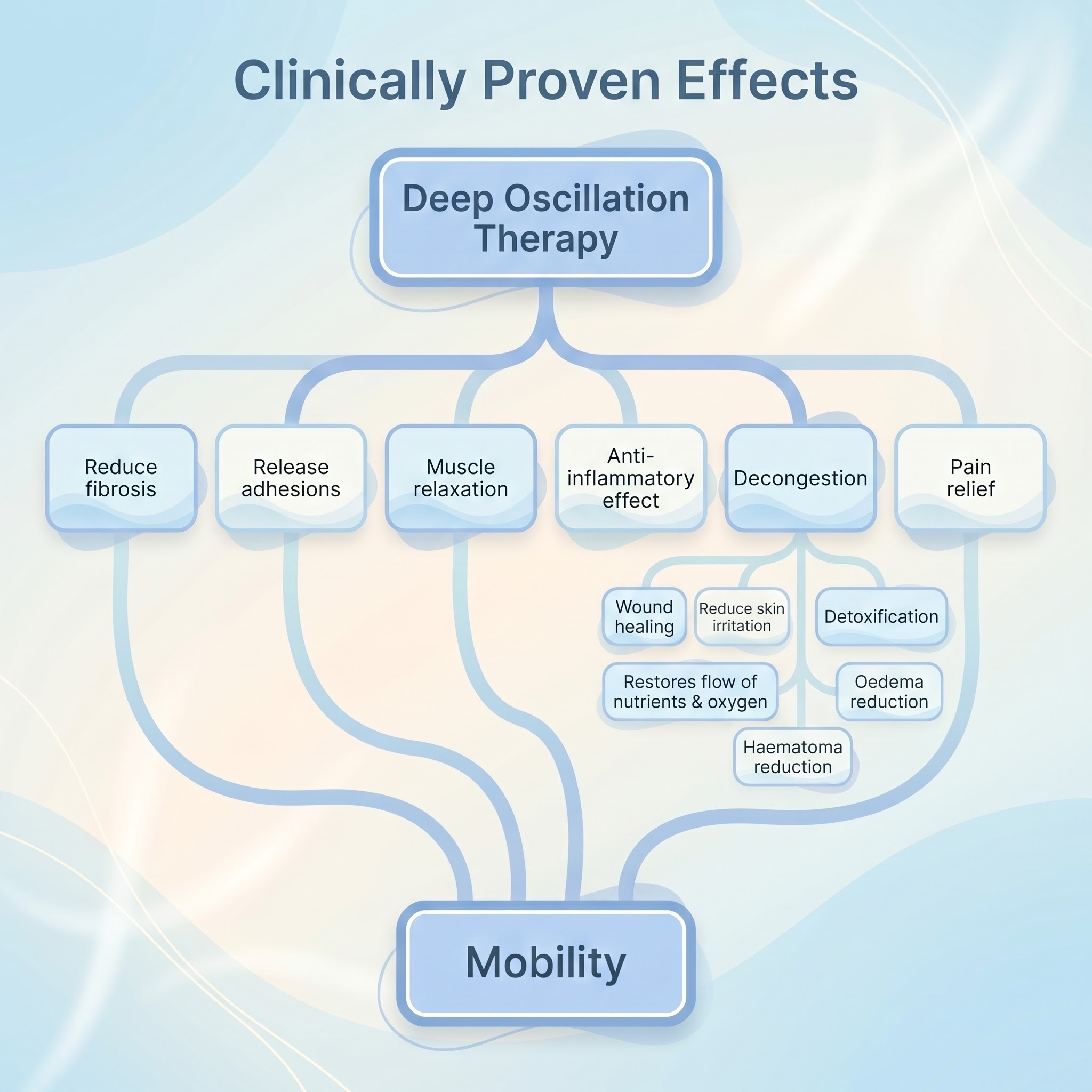
11. Clinically Proven Physiological Effects
The clinical efficacy of deep oscillation is supported by a robust body of research demonstrating significant physiological responses within the tissue. By intervening directly in the interstitial spaces of the connective tissue, the therapy initiates a cascade of primary and secondary healing mechanisms:
- Oedema and Haematoma Reduction: The resonant vibrations mechanically stimulate the interstitial spaces, enhancing lymphatic drainage and facilitating the rapid reabsorption of acute oedema and haematomas. Visual clinical proof utilising Indocyanine Green (ICG) fluoroscopy has definitively demonstrated that the gentle movement of the therapy applicator actively drives lymphatic fluid through the network. Recent 2025 trials demonstrate significant swelling reduction in early post-operative stages, such as ACL reconstruction, whilst earlier studies validate its efficacy in managing chronic conditions like lower-limb lymphoedema and lipoedema (Amore and Pineda, 2021; Oestervemb et al., 2025; Teo, Coulborn and Munnoch, 2016; Vladeva, Mihaylova and Panayotova, 2021).
- Pain Relief, Anti-Spasmodic and Anti-Inflammatory Effects: By reducing the release of inflammatory mediators (such as C-reactive protein, D-dimer, and the cytokine IL-8) and significantly decreasing the expression of TRPV1 pain receptors, the therapy produces a powerful anti-inflammatory effect. This provides rapid and long-lasting pain relief and anti-spasmodic benefits in both acute post-surgical trauma and chronic conditions (Boisnic and Branchet, 2013; Koleva, Ioshinov and Yoshinov, 2017; O'Brien and Watson, 2016; Portnov and Zabelina, 2002).
- Reduction of Fibrosis and Scar Tissue: The uninterrupted vibrating effect of the electrostatic impulses helps to disperse hardened, fibrotic tissue and prevent fibrotic conversion processes. This mechanism has proven highly effective in softening severe contractures, improving the pliability of burn scars, and managing fibrocystic breast disease (Hernández Tápanes et al., 2018; Pogorzelska et al., 2017).
- Wound Healing: By improving local microcirculation and restoring the flow of essential nutrients and oxygen to the tissues, the therapy significantly accelerates secondary wound healing processes, including the dynamic healing of burns (Hernández Tápanes et al., 2009; Mikhalchik et al., 2005).
- Muscle Relaxation and Mobility Restoration: The gentle tissue agitation effectively lowers muscle tone, relieves spasms, and significantly improves range of motion (ROM) and flexibility (von Stengel et al., 2018).
The cascade of primary and secondary biological responses generated by the therapy, which ultimately culminate in the restoration of patient mobility, is summarised below (Figure 4).
Figure 4. The clinically proven physiological effects of DEEP OSCILLATION® therapy.
12. Conclusion
In reviewing the modern physical therapy toolkit, it is clear that while therapies such as radiofrequency diathermy, ultrasound, and negative pressure therapy provide excellent targeted benefits through thermal or mechanical means, deep oscillation occupies a fundamentally unique position. By utilising the Johnsen-Rahbek effect to deliver a-thermic, intermittent electrostatic impulses, it is the only modality capable of penetrating 8 cm of tissue without requiring any physical downward pressure or suction.
This mechanism affords the therapy unparalleled safety and versatility, particularly in acute rehabilitation. Because it is completely heat-free, it overcomes the strict limitations of deep-heating thermotherapies, ensuring it can be safely applied directly over extreme oedema, passive metal implants, and prostheses. Furthermore, its ability to be delivered directly through the practitioner's gloved hands, or even over sterile films such as 3M Tegaderm for acute wound care, ensures strict infection control while offering exceptional adaptability.
Particularly in complex and delicate presentations such as Head and Neck Lymphoedema (HNL), where severe fibrosis occurs in areas that are notoriously difficult to massage, this gentle, non-invasive action proves invaluable. As evidenced by validated outcome measures such as the Glasgow Benefit Inventory, effective management of HNL yields profound physical and quality-of-life improvements for patients (Halliday, Gittins and Ahsan, 2020).
Notably for the practitioner, this application method provides significant ergonomic benefits. By eliminating the need to actively press a transducer probe or exert heavy manual force to reach deep tissue layers, it actively protects the therapist's hands and wrists from repetitive strain injuries while preserving vital tactile sensitivity.
Ultimately, while no single machine can ever replace the skilled hands of a trained practitioner, deep oscillation serves as an unparalleled extension of manual therapy. It seamlessly bridges the gap between acute trauma management, safe post-operative care, and sustainable at-home patient rehabilitation, securing its place as an essential, evidence-based tool in modern clinical practice.
13. Glossary of Clinical Terms
- A-thermic: A treatment modality that does not produce heat within the body's tissues.
- Diathermy: The use of high-frequency electromagnetic currents to generate deep endogenous heat within body tissues (e.g., radiofrequency diathermy, Shortwave).
- Endogenous Heat: Heat generated internally from within the body's own tissues, usually through the resistance of electrical or radiofrequency currents.
- Interstitial Spaces: The fluid-filled spaces situated between the cells of the connective tissues, which are the primary target area for deep oscillation.
- Johnsen-Rahbek Effect: The physics phenomenon of electrostatic attraction and friction, which forms the core operational basis of deep oscillation technology.
- Neuromuscular System: The vast network consisting of the nervous system and the muscles it controls, which is the primary target for conventional electrotherapies like TENS.
- Radiofrequency Diathermy (CRET): A form of endogenous thermotherapy utilising high-frequency radiofrequency currents (clinically known as Capacitive and Resistive Electric Transfer).
14. AI Disclosure Statement
In accordance with 2025-2026 academic and APA disclosure guidelines regarding the delineation of human versus artificial contributions: The core clinical concepts, specialised expertise, and overall structural framework of this article are entirely the original work of the author. Artificial Intelligence (AI) tools were utilised strictly as a secondary productivity aid for formatting, copyediting, and organising the academic citations to meet strict Harvard 2025-2026 referencing standards, ensuring the author's original information is presented in a clear, accessible, and academically rigorous manner.
15. References
Boisnic, S. and Branchet, M.C. (2013) 'Anti-inflammatory and draining effect of the deep oscillation device tested clinically and on a model of human skin maintained in survival condition', European Journal of Dermatology, 23(1), pp. 59-63. Available at: https://doi.org/10.1684/ejd.2012.1904 (Accessed: 22 April 2026).
Burgess, L. C., Immins, T., Swain, I. and Wainwright, T. W. (2019) 'Effectiveness of neuromuscular electrical stimulation for reducing oedema: a systematic review', Journal of Rehabilitation Medicine, 51, pp. 237–243. Available at: https://doi.org/10.2340/16501977-2529 (Accessed: 22 April 2026).
Dresing, K., Fischer, A.-C., Lehmann, W., Saul, D. and Spering, C. (2021) 'Perioperative and posttraumatic anti-edematous decongestive device-based negative pressure treatment for anti-edematous swelling treatment of the lower extremity - a prospective quality study', Int J Burn Trauma, 11(3), pp. 145-155. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8246067/ (Accessed: 22 April 2026).
Fatu, A. M., Ciobotaru, O. R., Daia, C., Sarbu, N., Zaharia, A. L. and Tanase, C. E. (2025) 'The Efficiency of Combined Capacitive and Resistive Energy Transfer (TECAR) Therapy and Low-Level Laser Therapy (LLLT) in Pain Reduction on Patients With Musculoskeletal Disorders: A Clinical Study', Cureus, 17(9). Available at: https://doi.org/10.7759/cureus.92670 (Accessed: 22 April 2026).
Ferriero, G., Coccetta, C.A., Sale, P., Ferrara, P.E., Specchia, A., Maccauro, G. and Ronconi, G. (2020) 'Capacitive and resistive electric transfer therapy in rehabilitation: a systematic review', International Journal of Rehabilitation Research, 42, pp. 106–111. Available at: https://doi.org/10.1097/MRR.0000000000000435 (Accessed: 22 April 2026).
(Accessed: 22 April 2026).
Hernández Tápanes, S., Socas Fernández, M. de J., Iturralde, Y. and Suáres Fernández, A. (2018) 'The Effect of deep oscillation Therapy in Fibrocystic Breast Disease. A Randomized Controlled Clinical Trial', International Archives of Medicine, 11(14). Available at: https://doi.org/10.3823/2555 (Accessed: 22 April 2026).
Iivarinen, J. T., Korhonen, R. K. and Jurvelin, J. S. (2013) 'Experimental and computational analysis of soft tissue mechanical response under negative pressure in forearm', Skin Research and Technology, 19(1), pp. e356-e365. Available at: https://doi.org/10.1111/j.1600-0846.2012.00652.x (Accessed: 22 April 2026).
Jahr, S., Schoppe, B. and Reisshauer, A. (2008) 'Effect of treatment with low-intensity and extremely low-frequency electrostatic fields (deep oscillation) on breast tissue and pain in patients with secondary breast lymphoedema', Journal of Rehabilitation Medicine, 40(8), pp. 645-650. Available at: https://pubmed.ncbi.nlm.nih.gov/18651079/ (Accessed: 22 April 2026).
Koleva, I. B., Ioshinov, B. R., and Yoshinov, R. D. (2017) 'Complex Analgesia (Infiltrations and deep oscillation) in Patients with Stump Pain and Phantom Pain after Lower Limb Amputation (Double-blind Randomised Controlled Trial of Efficacy)', Journal of Advances in Medicine and Medical Research, 22(11), pp. 1-17. Available at: https://doi.org/10.9734/JAMMR/2017/34198
(Accessed: 22 April 2026).
Lupowitz, L. G., Ramus, L., Delacour, F. and Johnson, K. (2025) 'TECAR Therapy: A Clinical Commentary on its Evolution, Application, and Future in Rehabilitation', International Journal of Sports Physical Therapy, 20(4). Available at: https://doi.org/10.26603/001c.130909 (Accessed: 22 April 2026).
Mikhalchik, E., Titkova, S., Anurov, M., Suprun, M., Ivanova, A., Trakhtman, I. and Reinhold, J. (2005) 'Wound Healing Effects of deep oscillation', 1st International Conference on Skin and Environment. Moscow-St. Petersburg, p. 71.
O'Brien, C.P. and Watson, A. (2016) 'deep oscillation Therapy in the Treatment of Lateral Epicondylalgia: A Pilot Randomized Control Trial', Journal of Sports Medicine & Doping Studies, 6(3). Available at: https://doi.org/10.4172/2161-0673.1000180
(Accessed: 22 April 2026).
Oestervemb, K., Trybulski, R., Szczygie?, E., Szczygielska-Babiuch, A., Kacprzak, B. and Hagner–Drengowska, M. (2025) 'deep oscillation therapy enhances early rehabilitation after ACL reconstruction: a randomized controlled trial', Journal of Rehabilitation Medicine, 57, jrm44416. Available at: https://doi.org/10.2340/jrm.v57.44416 (Accessed: 22 April 2026).
Pogorzelska, J. A., Zaglaniczny, D., Zmyslna, A., and Kiebzak, W. (2017) 'Observation of deep oscillation usage and its effectiveness on burn scars—case report', Medical Studies/Studia Medyczne, 33(1), pp. 46–50. Available at: https://www.physiopod.co.uk/assets/pdfs/BURNS%20SCARS.pdf (Accessed: 22 April 2026).
Sinclair, A. V. S., Garty, F. L. R., Smith, J. R. and Shipman, A. R. (2023) 'Is it safe for patients with metal implants to have iontophoresis treatment?', Clinical and Experimental Dermatology, 48(7), pp. 759–764. Available at: https://doi.org/10.1093/ced/llad07z (Accessed: 22 April 2026).
Thaler, E., Toledo, F. and Korte, H. (2017) 'Can Direct Current Electrotherapy Be Used for Patients With Orthopedic Implants?', Geriatric Orthopaedic Surgery & Rehabilitation, 8(1), pp. 44-48. Available at: https://pubmed.ncbi.nlm.nih.gov/28255511/
(Accessed: 22 April 2026).
Vladeva, E., Mihaylova, M. and Panayotova, L. (2021) 'DEEP OSCILLATIONS- REDUCING EDEMA AND IMPROVING KINESIOLOGY IN THE EARLY STAGES AFTER KNEE JOINT ARTHROPLASTY', Journal of IMAB, 27(1), pp. 3577-3581. Available at: https://doi.org/10.5272/jimab.2021271.3577 (Accessed: 22 April 2026).
von Stengel, S., Teschler, M., Weissenfels, A., Willert, S. and Kemmler, W. (2018) 'Effect of deep oscillation as a Recovery Method after Fatiguing Soccer Training: A Randomized Cross-Over Study', Journal of Exercise Science and Fitness, 16(4), pp. 112-117. Available at: https://doi.org/10.1016/j.jesf.2018.10.004 (Accessed: 22 April 2026).