Lymphoedema Responds Favourably to Deep Oscillation and a Wholistic Treatment Approach
Christine Talbot provides a wholistic, inspiring and effective treatment approach for the reduction and management of Lymphoedema aiding and empowering self care.
Background
In 1994, aged 37, Mrs R was diagnosed with Multiple Sclerosis; her sister is also affected and is wheelchair bound.
Mrs R experienced a loss of clear vision, a loss of balance, her legs became weak with a loss of power to her left leg and a loss of neuro transmission to her right leg. The symptoms worsened with stress related attacks causing increased fatigue, numbness to the right hand, bladder hyperactivity with frequent urinary tract infections, less resistance to infection and a change in memory and concentration. She was prescribed steroids and used to self-inject with Copaxone 2010 to 2014. Advances in better medication, Fingolimod 0.5 mg daily (2014 to present day) have halted the progression of the disease and Mrs R was otherwise fit and doing well.
In 2021, following her first COVID vaccination, Mrs R experienced pain in her inguinal lymph nodes:
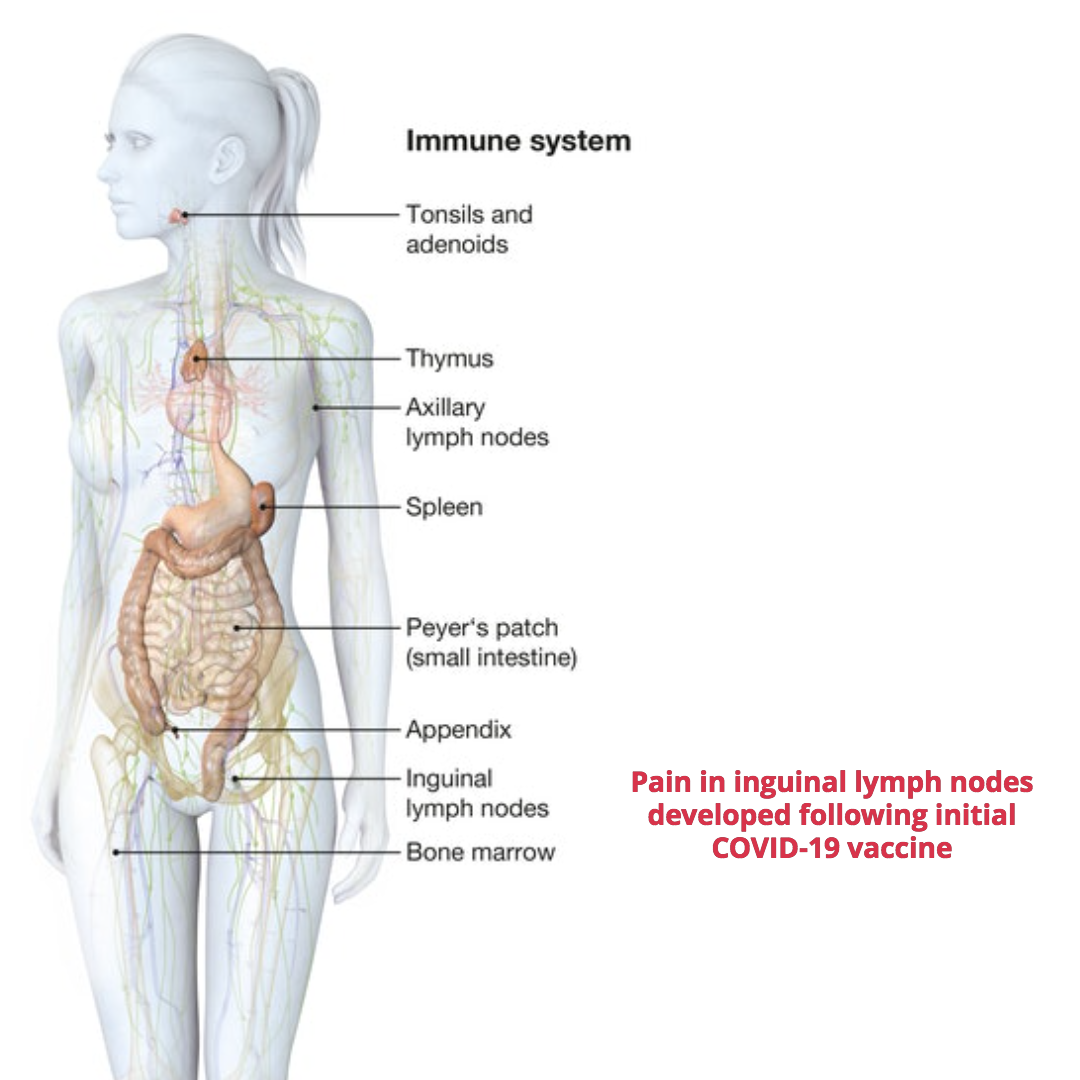
Following the second vaccine, Mrs R's right leg began to swell, it was very painful and became noticeably larger in circumference in comparison to her left leg. This change impacted normal mobility and altered further Mrs R’s quality of life she had adapted to with multiple sclerosis.

Clinical investigations
- CT (computed tomography) scan of abdomen and pelvis did not identify any intra-abdominal or pelvic cause for the oedema in the right leg.
- Venous ultrasound uses sound waves to produce images of the veins in the body, commonly used to search for blood clots, especially in the veins of the leg. Nothing irregular was found.
- Lymphoscintigraphy – “is a powerful diagnostic imaging modality using radioactive tracers to identify abnormalities within the lymphatic system [1]. The result was non-defining and vague with regards to lymphatic vessels and nodes, suggesting a density but without evaluative reason. However, a Lymphoedema diagnosis was made.
- Spinal Scan/MS review with MS Consultant ruled out any suspicion of MS causing the new swelling in the right leg.
Mrs R reported the adverse effect to Coronavirus Yellow Card reporting site and directly to the pharmaceutical company producing the vaccine. The company have not stated having received any other notification of this type of reaction. Manual lymphatic drainage (MLD) has been recommended to help reduce and maintain symptoms and to be fitted with compression stockings to control swelling of the right leg.
Referral for Treatment
Following a referral through PhysioPod, Mrs R attended for Manual Lymphatic Drainage (MLD) with the addition of Deep Oscillation Therapy (as recommended by a Chartered Physiotherapist who was consulted on the case and knew of the clinical effects of Deep Oscillation in Lymphoedema management).
Clinical Presentation
Mrs R is a tall, slim, fit, very active sixty-three-year-old lady, she uses a stick for balance reassurance as she has a left hip replacement (April 2018). Mrs R’s right leg was completely solid, like a brick wall, particularly around the knee which was inflexible with skin changes, the right foot was swollen with a pronounced lymph lake and positive Stemmer, there was slight movement at the ankle, which was sufficient for driving an automatic car. The abdominal, pelvic, mons pubis area was significantly engorged.
Treatment began on 19th July 2021
- Deep Oscillation within the frequency range 100 Hz to 160 Hz for the entire treatment session [2-26]
- Quantum Wave Laser - placed in the right groin area for 6 mins groin, 6 mins popliteal on a lymphatic setting in order to soften areas [27-31]
- Manual Lymphatic Drainage (MLD)
- Multi-layer Lymphoedema bandaging (MLLB)
- Bowen Techniques
- Specific exercises to aid lymphatic flow
- Supplement advice
- Self Lymphatic Drainage instruction
- Adjunctive therapy modality advice
On the first session, the upper thigh responded well and movement became apparent along the adductor canal, plus more movement occurred at the ankle.
However, the knee remained rigid, so manipulation of the patella (in all directions) was demonstrated to aid drainage at the knee.
- The Bowen 'knee and lower leg procedure' was carried out with an encouraging response with greater all-round ankle rotation.
- The benefits and physics of multi-layer Lymphoedema bandaging (MLLB) were explained with Mrs R. I anticipated quicker results would be achieved with this approach and taught Mrs R how to self-bandage. As Mrs R has a horse, she had a head start on the application of bandaging and easily got to grips with how to apply the method to her own leg.
- Various exercises were discussed and demonstrated to encourage more limb flexibility and to improve muscle mass and nerve stimuli. We discussed the benefits overall to reinitiating muscle mass by the use of a Power Plate, explaining how the big VibraGyms were designed by Russians for Astronauts returning from Space with little muscle mass. The effect of standing on a vibrating plate automatically causes muscle tension to maintain balance and increases core stability.
- We discussed the Revitive machine, for strengthening blood vessels and calf muscles in the lower leg.
- Self-massage techniques were shown to specific areas, in particular the lymph nodes in the groin, hip and behind the knee
Mrs R left feeling much encouraged by the array of possibilities open to her to take control and self-manage and was delighted to see and feel the remarkable effects of deep oscillation within the first appointment.
Results/Ongoing Treatment

Above Knee Limb Measurements in circumference from the onset of swelling to now :-
Right leg, (at its worst) 490mm, now approximately 440mm, left leg 380mm.
Appointments are on-going once or twice a week, the limb above the right knee now measures 440 mm.
Mrs R is now using both a small power plate and a Revitive machine, in a short space of time these have really started to re shape her leg.
On the second appointment, the right leg was pre-bandaged while the rest of the body was treated, the bandage was then removed to treat the right leg. This gave Mrs R an opportunity to familiarise herself with the look and feeling of the bandage, plus she took photographs. She was impressed with the limb changing shape and softening of her leg. I compiled a prescriptive bandage list for her GP to prescribe so daily bandaging could commence:
- ComfiFast™ Yellow Line stockinette
- Comprilan short stretch 8 x 1, 10 x 2, 12 x 2 bandages and now she leaves each time with a modified Lymphoedema bandage to her right leg and continues with bandaging at home, modified because Mrs R is a very active ambulant person, plus she has to drive home so the bandage cannot be too dense. Other than a slight setback between appointment three and four when the left prosthetic hip dislocated requiring hospitalisation for a manipulation under anaesthetic (MUA), progress is ongoing and very positive. At Mrs R’s last appointment, she was measured for a Comfiwave leg support from hadhealth.com, as this will be very beneficial for night wear but also as an addition to bandaging, where it might not be appropriate to be so encased. I have suggested also taking a very good quality Probiotic to ward off infection as good gut bacteria is invaluable against bacterial infections. Mrs R has had several repeat episodes of urinary tract infections which never entirely resolve with antibiotics, I have suggested Waterfall D Mannose which is very effective in dealing with long term chronic UTI’s.
- I have suggested getting a ‘Roly” from Sigvaris, a simple applicator for donning hosiery, however it is an excellent tool for a patient to push fluid up the whole circumference of the limb.
So impressed is Mrs R with Deep Oscillation, she has just ordered her own personal unit. I think this will be invaluable, not only in light of the Lymphoedema but also it might prove very beneficial for her multiple sclerosis, plus she can treat her horse as and when required.
Practitioner Conclusion
I cannot imagine how it must feel to suddenly be confronted with such an adverse, alarming and unrecognised response to the Coronavirus vaccine, especially when already dealing with the complexities and physical demands of an auto immune condition which under normal circumstances could at any time destabilise. It is interesting to note when Mrs R was first diagnosed with Multiple Sclerosis her right leg had a loss of neuro transmission. The involuntary pulsation of the lymphatic vessels is under the control of the autonomic nervous system causing an involuntary pulsation of the vessels which initiates the propulsion of the lymph obligatory load in a twenty-four-hour period towards the heart combined with muscular activity against the vessels. I wonder if it is possible that the involuntary autonomic neurological function of the right leg has been affected by the vaccine causing an abnormal enlargement of the right leg due to a failure of normal lymphatic flow.
ABOUT DEEP OSCILLATION®
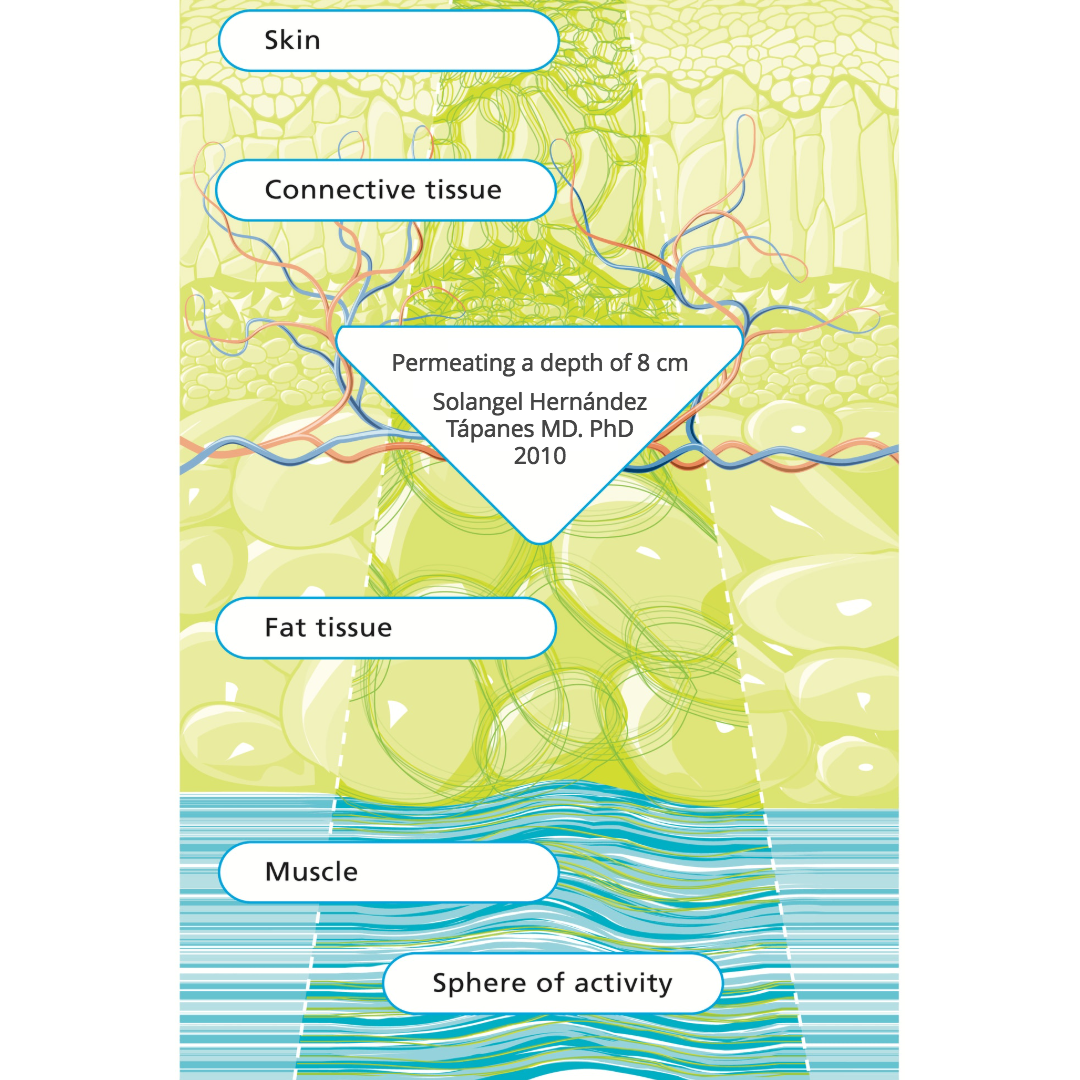
In contrast to externally applied, mechanical forms of therapy, (e.g. vibration), the therapy effect of DEEP OSCILLATION® takes place in the tissue itself and works through the entire depth of the tissue layers (skin, connective tissue, subcutaneous fat, muscles, blood and lymph vessels)
DEEP OSCILLATION® helps in speeding up and improving wound healing processes. Through the oedema-reducing and anti inflammatory effect, the local metabolic elimination and alimentation is improved in all tissue layers, whereby tissue regeneration and wound closure are encouraged on many levels. This is documented by the significant improvement in planimetric and biochemical parameters of the wound healing.
Because of the non-invasive, non-traumatic, gentle nature of this therapy, very early possibilities of application are possible following injury and from Day One post operatively. Chronic conditions can also be worked upon with effective results.
About Low level laser therapy (LLLT)
"Low level laser therapy (LLLT) is the use of low energy laser light in injuries and wounds in order to improve wound healing, reduce inflammation and alleviate pain. The laser light is monochromatic, coherent and in the red or near infrared spectrum (600 nm – 1000 nm). It is applied at low power density (1 mW to 500 mW/cm2) (“low energy laser”).
In contrast to other medical laser applications LLLT is not a thermal method (i.e. surgical lasers), but produces photochemical effects in the tissue in a similar way to photosynthesis in plants. LLLT is simple to use, effective and cost-efficient and free of side effects. Treatment takes a few minutes and depending on the indication is repeated at longer or shorter intervals and in accordance with healing success. The success of LLLT is based on the following general action principles: tissue regeneration, inhibition of inflammation, alleviation of pain, improvement in circulation, reduction in swelling" Low-Level-Laser-Therapy (LLLT) in Chronic Wounds - Ludwig-Maximilian University Munich, Germany.
References
- Ranzenberger LR, Pai RB. Lymphoscintigraphy. [Updated 2020 Sep 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-.
- Atashkhoei S., Fakhari S. (2016): Management of Breast Cancer Related Lymphoedema. Crescent Journal of Medical and Biological Sciences 3 (4), 111-112.
- Brenke R. - Therapie des Lymphödems EHK 2021; 70: 138-144 DOI - 10.1055/a-1477-817
- Brenke R., Freund R., Strößenreuther RHK (2010): Adjuvant physical therapy for lymphedema and selected comorbidities of the musculoskeletal system. In: Földi M., Földi E. (Ed.): Textbook Lymphology. 7th ed., Elsevier GmbH, 508.
- Brenke R., Siems W. (1996): Adjuvant Therapy for Lymphedema. Lymphol 20, 25-29.
- Flemming D. (2016): The technique of deep oscillation. Lymph self-help, 22-23.
- Gasbarro V., Bartoletti R., Tsolaki E., Sileno S., Agnati M., Coen M., Conti M., Bertaccini C. (2006): Ruolo dell'oscillazione profonda (Hivamat® 200) nel trattamento fisico del linfedema degli arti. La medicina estetica 30 (4), 473-478. English title: The role of deep oscillation therapy (Hivamat® 200) in the physical treatment of the lymphoedema of the limbs.
- GDL (Society of German-speaking Lymphologists) u. DGL (German Society of Lymphology) (2017): AWMF-S2k Guideline "Diagnosis and Treatment of Lymphedema" (AWMF Reg. No. 058-001).
- Jahr S, Schoppe B, Reisshauer A. Effect of treatment with low-intensity and extremely low-frequency electrostatic fields (Deep Oscillation) on breast tissue and pain in patients with secondary breast lymphoedema. J Rehabil Med. 2008 Aug;40(8):645-50. doi: 10.2340/16501977-0225. PMID: 19020698.
- J of IMAB 2016 Jul-Sep;22(3):1248-1252 Improving the quality of life through effects of treatment with low intensity, extremely low frequency electrostatic field with DEEP OSCILLATION® in patients with breast cancer with secondary lymphedema to patients treated with standard lymph equipment. Atanas Petkov1 Corresponding Autor, Yana Kashilska2, Angel Uchikov1, Dean Batzelov3,
- Jui Chu Y. (2017): HIVAMAT 200. In: Jui Chu Y. (Ed.): What Can Physical Therapy Do After Breast Cancer Surgery. CARE, 187-188. German translation: What can physical therapy do after breast cancer surgery.
- Kraus R. (2014): Intensive lymphatic drainage through deep oscillation. LYMPH & Health 2, 6-8.
- Lipiska A., Opuchlik A. (2014): Fizycoterapia w onkologii. In: ?liwi?ski Z., Siero? A. (Ed.): Wielka Fizjoterapia. Elsevier GmbH, 289-294. English title: Physical Therapy in Oncology.
- Mortimer P., Levine G. (2019): Let's Talk Lymphoedema, The Essential Guide to Everything You Need To Know
- Reisshauer A., Pögel S. (2010): Treatment of Secondary Arm Lymphodema in Breast Cancer. Gynecol. prax. 34, 489-499.
- Reißhauer A., Auler S., Bieringer S., year S. (2009): physical decongestive therapy. In: Reißhauer A., Auler S., Bieringer S., year S. (Ed.): Compendium of the lymphological compression supply. Federal School of Orthopedic Technology, 42-57.
- Schingale F.-J. (2006): Head, breast and genital lymphedema - a special challenge for the lymphatic therapist. vasomed 1, 30-31.
- Talbot C. (2011): Lymphoedema Support Network periodical 'Lymphline', Spring Issue, Deep Oscillation for lymphoedema
- Teo I., Coulborn A., Munnock DA (2016): Use of the HIVAMAT® 200 with manual lymphatic drainage in the management of lower limb lymphoedema and lipoedema. Journal of Lymphoedema 11 (1), 49-53
- Theys S., Deltombe T., Legrand C., Hanson P. (2008): Manual Drainage with or without DEEP OSCILLATION® in Lower Extremity Oedema. J Rehabil Med Suppl 47, 62.
- Kraus R. (2014): Intensive lymphatic drainage through deep oscillation. LYMPH & Health 2, 6-8.
- Talbot C. (2011): Lymphoedema Support Network periodical 'Lymphline', Spring Issue, Deep Oscillation for lymphoedema
-
Mosca, R. C., et al. (2019). "Photobiomodulation Therapy for Wound Care: A Potent, Noninvasive, Photoceutical Approach." Adv Skin Wound Care 32(4): 157-167.
-
Machado, R. S., et al. (2017). "Low-level laser therapy in the treatment of pressure ulcers: systematic review." Lasers Med Sci 32(4): 937-944.
-
Tchanque-Fossuo, C. N., et al. (2016). "A systematic review of low-level light therapy for treatment of diabetic foot ulcer." Wound Repair Regen 24(2): 418-426.
-
Kuffler, D. P. (2016). "Photobiomodulation in promoting wound healing: a review." Regen Med 11(1): 107-122.
