Lipoedema as a Connective Tissue Disorder: The 2026 PhysioPod® UK Independent Review
For our readership of patients and professionals, this 2026 review brings together the latest research to support both clinical practice and daily self-care, signposting to the excellent support groups in the Lipoedema Community and the professional registers of highly-skilled private practitioners.
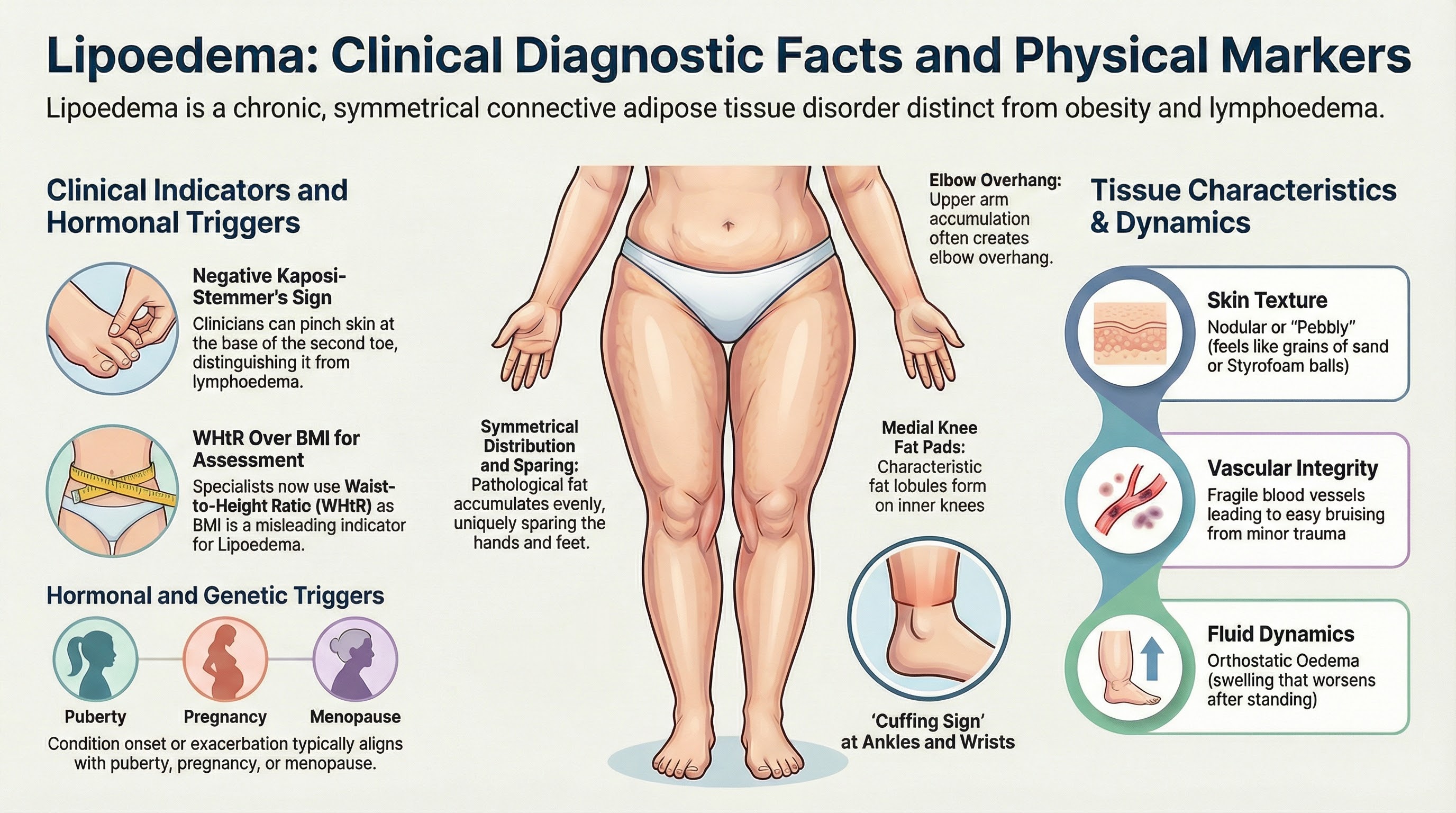
Figure 1: Understanding Lipoedema: A visual summary of the defining physical characteristics, clinical diagnostic markers
Copyright 2026 PhysioPod® UK Ltd.
Scan this QR code (or ask your GP to) with smartphone camera to read the digital version of this article, complete with clickable scientific references and interactive resource links
Imprint and Publication Details
Published by: PhysioPod® UK Ltd, Daybrook Nottingham, Nottinghamshire, NG5 6AS United Kingdom
Contact Information: Telephone: +44 (0)115 916 7685 Email: enquiries@physiopod.co.uk Website: www.physiopod.co.uk
Company Registration: Co. Reg: 5871545 | VAT No: GB-893005132
Copyright & Sharing: © Copyright 2026 PhysioPod® UK Ltd. This publication is intended as an open educational and clinical resource. We encourage the sharing of this information. It may be freely reproduced, distributed, or transmitted in any form, provided that PhysioPod® UK Ltd is clearly credited as the original publisher and source.
Medical Disclaimer: The content, text, graphics, and data offered herein are provided solely to educate readers on health care and medical issues. This document is intended for general educational and informational purposes only and should not be considered or used as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified healthcare provider with any questions you may have regarding a medical condition. Reliance on the content within this publication is solely at your own risk.
Table of Contents
List of Figures and Multimedia
For many women living with lipoedema, the journey to finding effective relief from heavy limbs, swelling, and varying degrees of tissue tenderness can be exhausting. While the presence and intensity of pain vary widely from person to person, and are not an absolute requirement for diagnosis (Herbst et al., 2021; Kruppa et al., 2026), the physical and emotional burden of the condition is universally recognised. Traditional diet and exercise often fail to impact lipoedema tissue, leaving many searching for a non-invasive solution that actually works.
As described by Duhon et al. (2022), lipoedema is a chronic, progressive connective adipose tissue disorder that almost exclusively affects women. It is characterised by a symmetrical, disproportionate accumulation of abnormal fat that is biologically distinct from "normal" fat (Straub et al., 2025). While the condition most commonly affects the hips, buttocks, and legs, it also affects the arms in approximately one-third of cases (Chachaj et al., 2023).
Despite historical misunderstandings, the condition is now officially recognised globally by the World Health Organisation as a distinct disease entity under the ICD-11 classification system (code EF02.2 for Lipoedema, and BD93.1Y for lipo-lymphoedema). Furthermore, to support practical clinical management and accurate staging, it has now been granted highly specific diagnostic codes in the newly updated 2026 ICD-10-CM (the E88.2 series). This guarantees that non-specific swelling, or simple adiposity, no longer categorises the condition.
To underpin this new era of recognition, 2026 saw the publication of the landmark Lipedema World Alliance (LWA) Delphi Consensus in Nature Communications (Kruppa et al., 2026). Formulated by a panel of specialists from 19 countries, this historic paper established 59 unified clinical agreements. It officially defined lipoedema as a distinct subcutaneous adipose tissue disease, formally separated it from lifestyle-induced obesity, and validated both conservative management and surgical intervention. This consensus provides the ultimate, evidence-based framework for the modern treatment strategies discussed in this article.
Complementing this newly established clinical framework, the clinical landscape of lipoedema diagnosis is also shifting rapidly. While diagnosis has historically relied purely on physical examination, a newly accepted 2026 manuscript published on behalf of the British Association of Dermatologists reveals that an 'adipocytokine signature'—utilising specific blood biomarkers such as fibroblast growth factor 21 (FGF21) and chemerin—can significantly improve diagnostic accuracy. This breakthrough means that an objective blood test to support clinical diagnosis is finally on the horizon, providing immense hope for patients and perfectly complementing the multimodal treatment framework discussed in this review.
- Symmetrical Distribution: The abnormal fat accumulates evenly on both sides of the body (Dal’Forno-Dini et al., 2025).
- Diagnostic Markers: Clinicians look for a negative Kaposi-Stemmer’s sign and an absence of pitting oedema to help distinguish it from standard lymphoedema (Kruppa et al., 2026). Furthermore, because BMI is a poor indicator for lipoedema, specialists now advise using the Waist-to-Height Ratio (WHtR) to properly assess patient health (Kruppa et al., 2026).
- The "Cuffing Sign": A defining characteristic, noted by Shavit et al. (2018) and reaffirmed by the 2026 Global Consensus, is that the fat distribution stops abruptly at the ankles and wrists, meaning the hands and feet remain unaffected and "spared"
- Arm Involvement & Elbow Overhang: When the arms are affected, the disproportionate fat typically accumulates heavily in the upper arms. As confirmed by the 2026 Global Consensus, this can create a distinct tissue overhang that stops abruptly at the elbows, though in some cases it extends to the forearms (Kruppa et al., 2026)
- Inner Knee Fat Pads & Tissue Overhang: The formation of distinct fat pads, lumps, or lobules on the inner (medial) sides of the knees is a very common and characteristic physical sign of the condition. For many patients, this accumulation creates a pronounced tissue overhang that stops abruptly at the knee (Tugral and Bakar, 2019; Dal'Forno-Dini et al., 2025)
- Hormonal and Genetic Roots: Symptoms typically onset or exacerbate during periods of hormonal fluctuation, such as puberty, pregnancy, or menopause. The 2026 Global Consensus confirms that these hormonal changes are a primary trigger for the disease's progression, and additionally highlights a strong hereditary component, with the condition frequently observed among female family members (Kruppa et al., 2026).
- Varying Degrees of Pain and Tenderness: While symptoms can range from a mild feeling of heaviness to spontaneous throbbing, affected areas can often be sensitive to the touch. The 2026 Global Consensus confirms that while physical pressure sensitivity is a central symptom for many, the intensity varies widely from person to person, ranging from mild discomfort to severe, chronic pain (Kruppa et al., 2026). For those experiencing the more severe end of this spectrum, the chronic nature of the pain, combined with the psychosocial burden of the condition, often leaves patients in a prolonged state of physiological stress or anxiety (Luta et al., 2025). This heightened stress response can manifest in secondary physical symptoms, such as chronic muscle tension in the jaw or shoulders, further complicating the patient's physical discomfort (Kruppa et al., 2026; Luta et al., 2025).
- Easy Bruising: The small blood vessels in lipoedema tissue are fragile, leading to frequent and easy bruising even from minor trauma, a finding confirmed by Duhon et al. (2022) and reinforced by the Lipedema World Alliance (2026).
- Nodular Skin Texture: Unlike standard adipose tissue, affected skin often feels uneven, nodular, or "pebbly" to the touch. The British Journal of Nursing describes this distinct texture as feeling like "grains of sand" or "Styrofoam balls" beneath the skin (Crouch, 2025).
- Swelling: Patients frequently experience orthostatic oedema (swelling that worsens during the day or after standing), especially in the legs (Shavit et al., 2018).
- Impact on Wellbeing: Living with lipoedema carries a heavy psychosocial burden. A 2025 retrospective study from a Swiss referral centre found a high prevalence of anxiety and depression among patients, emphasising that psychological support must be a core pillar of the standard of care (Luta et al., 2025).
- Resistance to Standard Weight Loss: Because lipoedema fat is pathological and highly fibrotic, it is notoriously resistant to traditional calorie restriction and standard exercise. However, a major 2025/2026 clinical paradigm shift has proven that intensive, targeted anti-inflammatory approaches (such as strict ketogenic or low-carbohydrate diets) combined with physical activity can successfully reduce systemic inflammation and promote significant localised fat loss in the limbs (Cifarelli et al., 2024; Faria et al., 2026)
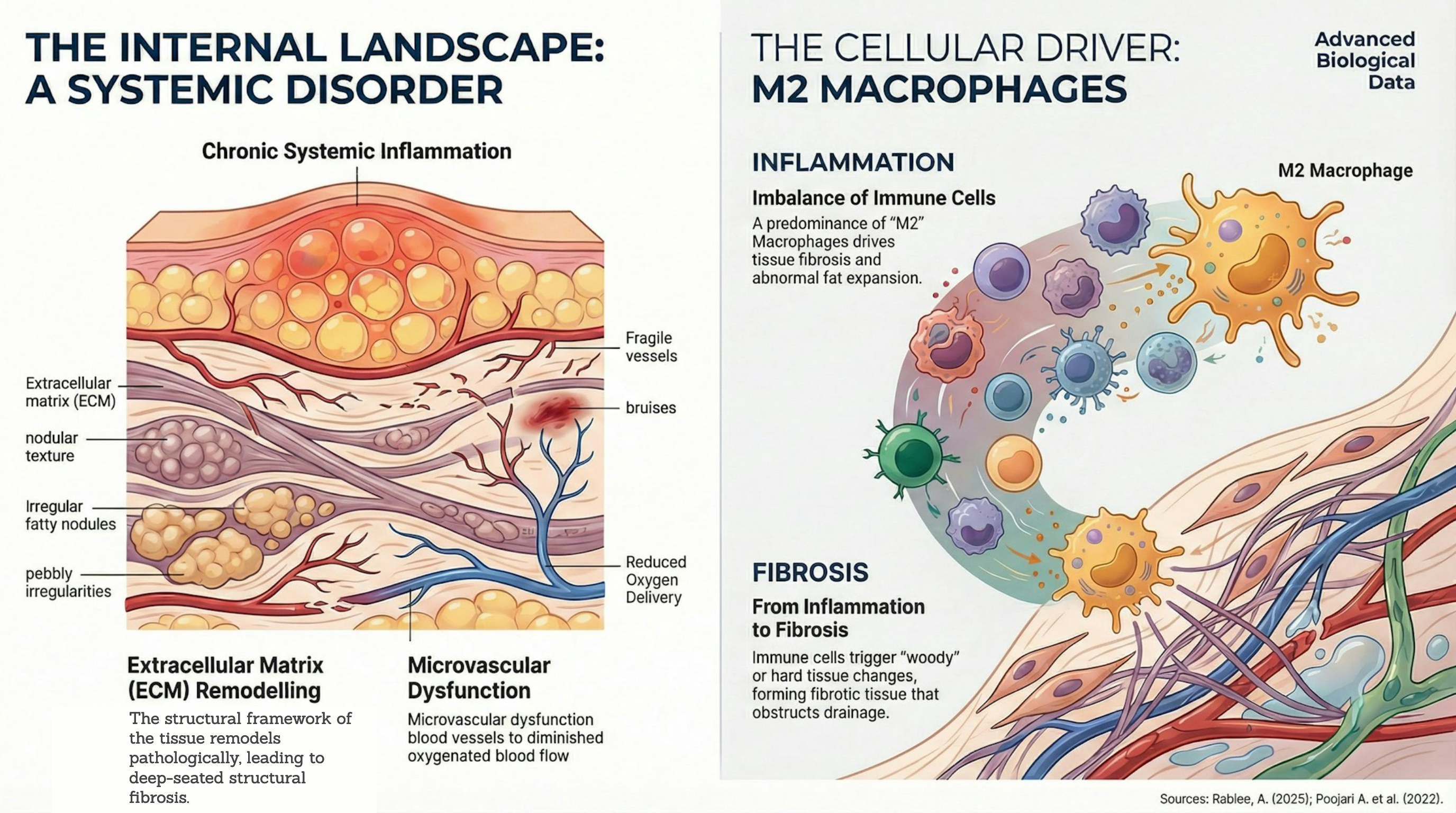
Figure 2: The Internal Landscape of Lipoedema. A visual representation of the advanced multi-omics data demonstrating that lipoedema is fundamentally a systemic disorder. On the left, the tissue cross-section highlights extracellular matrix (ECM) remodelling, chronic systemic inflammation, and microvascular dysfunction—which leads to fragile vessels, bruising, and reduced oxygen delivery. On the right, the cellular driver is revealed: an imbalance of immune cells, where a predominance of 'M2' macrophages triggers "woody" fibrotic tissue changes that obstruct natural fluid drainage and drive abnormal, disproportionate fat expansion. Sources: Rabiee, A. (2025); Poojari A. et al. (2022). © Copyright 2026 PhysioPod® UK Ltd.
Advanced multiomics research highlighted by Straub et al. (2025) and Dal'Forno-Dini et al. (2025) proves lipoedema is fundamentally a systemic disorder involving extracellular matrix remodelling, chronic inflammation, an imbalance in immune cells (macrophage polarisation), and microvascular dysfunction (Duhon et al., 2022; Poojari et al., 2022; Rabiee, 2025). Recent analyses reveal a distinct predominance of 'M2' macrophages driving tissue fibrosis and abnormal fat expansion. Furthermore, cutting-edge research highlights the presence of overactive mast cells within the tissue, which significantly contribute to the condition's characteristic pain, swelling, and chronic immune activation (Herbst, 2025). While diagnosis has historically relied purely on physical examination, this landscape is rapidly shifting. A newly accepted 2026 manuscript published on behalf of the British Association of Dermatologists demonstrates that an 'adipocytokine signature' can significantly improve diagnostic accuracy for people living with the condition (Mühlberg et al., 2026). Researchers discovered that certain blood biomarkers, notably fibroblast growth factor 21 (FGF21) and chemerin, serve as robust, independent predictors of lipoedema, outperforming conventional metabolic indicators (Mühlberg et al., 2026). Combining these biomarkers could soon help doctors objectively confirm their diagnosis, which would be a valuable addition to the physical exam.
Resistance to Lifestyle Changes: While lipoedema tissue is resistant to calorie restriction alone, the latest S2k Guidelines (Faerber et al., 2024) specifically recommend ketogenic or isocaloric Mediterranean diets. These approaches aim to lower insulin levels and reduce the systemic inflammation that drives pain, rather than focusing solely on weight loss.
Resistance to Lifestyle Changes: While lipoedema tissue is resistant to calorie restriction alone, the latest S2k Guidelines (Faerber et al., 2024) specifically recommend ketogenic or isocaloric Mediterranean diets. These approaches aim to lower insulin levels and reduce the systemic inflammation that drives pain, rather than focusing solely on weight loss.
The clinical landscape of lipoedema management is rapidly evolving, increasingly embracing systemic treatments such as the anti-inflammatory and anti-fibrotic benefits of GLP-1 medications (Viana et al., 2025; Cifarelli, 2025) alongside microcirculation-boosting supplements like Pycnogenol (Netto et al., 2025).
However, while these systemic drugs are highly effective at managing chronic inflammation and metabolic burden—with recent literature highlighting dual-agonists like Tirzepatide as potential "disease-modifying therapies" capable of biochemically targeting adipose tissue fibrosis (Viana et al., 2025)—they cannot mechanically break apart already established, hard nodular masses. To address this existing structural induration, targeted physical and surgical interventions are required. Evidence suggests that advanced conservative modalities like Deep Oscillation Therapy and Extracorporeal Shock Wave Therapy (ESWT) can safely penetrate the tissue to soften deep-seated induration and connective tissue restrictions (Siems et al., 2005; Hernández Tápanes et al., 2010; Almendras et al., 2024; Fickling, 2026). Although large-scale studies specifically for lipoedema are still evolving, robust evidence from a randomised, controlled clinical trial on comparable fibrotic connective tissue models—such as fibrocystic breast disease—demonstrates that Deep Oscillation effectively reduces both pain and deep tissue induration (Hernández Tápanes et al., 2018). Furthermore, deeper manual techniques like myofascial release can help mobilise these adhesions, while lymph-sparing liposuction remains the only definitive method to physically extract the nodular tissue entirely (Kruppa et al., 2026; Dal'Forno-Dini et al., 2025). Because of this, hands-on physical therapies and surgical interventions remain absolutely essential counterparts to effective disease management.
To address this established structural fibrosis, specialists emphasise that successful management absolutely requires a "team effort" via a multimodal protocol (Viana et al., 2025; Dal'Forno-Dini et al., 2025; Forner-Cordero et al., 2021). Within this framework, targeted physical and surgical interventions remain essential counterparts to pharmacological care. Advanced conservative modalities like Deep Oscillation Therapy and Extracorporeal Shock Wave Therapy (ESWT) safely penetrate the tissue to soften deep-seated hardening and fibrotic restrictions (Siems et al., 2005; Hernández Tápanes et al., 2010; Almendras et al., 2024; Fickling, 2026). Furthermore, deeper manual techniques like myofascial release help mobilise these adhesions, while lymph-sparing liposuction remains the only definitive method to physically extract the nodular tissue and fibrotic extracellular matrix entirely (Kruppa et al., 2026; Dal'Forno-Dini et al., 2025). By combining pharmacological agents, mechanical strategies, and potential surgical interventions, clinicians can effectively target every layer of the pathology.
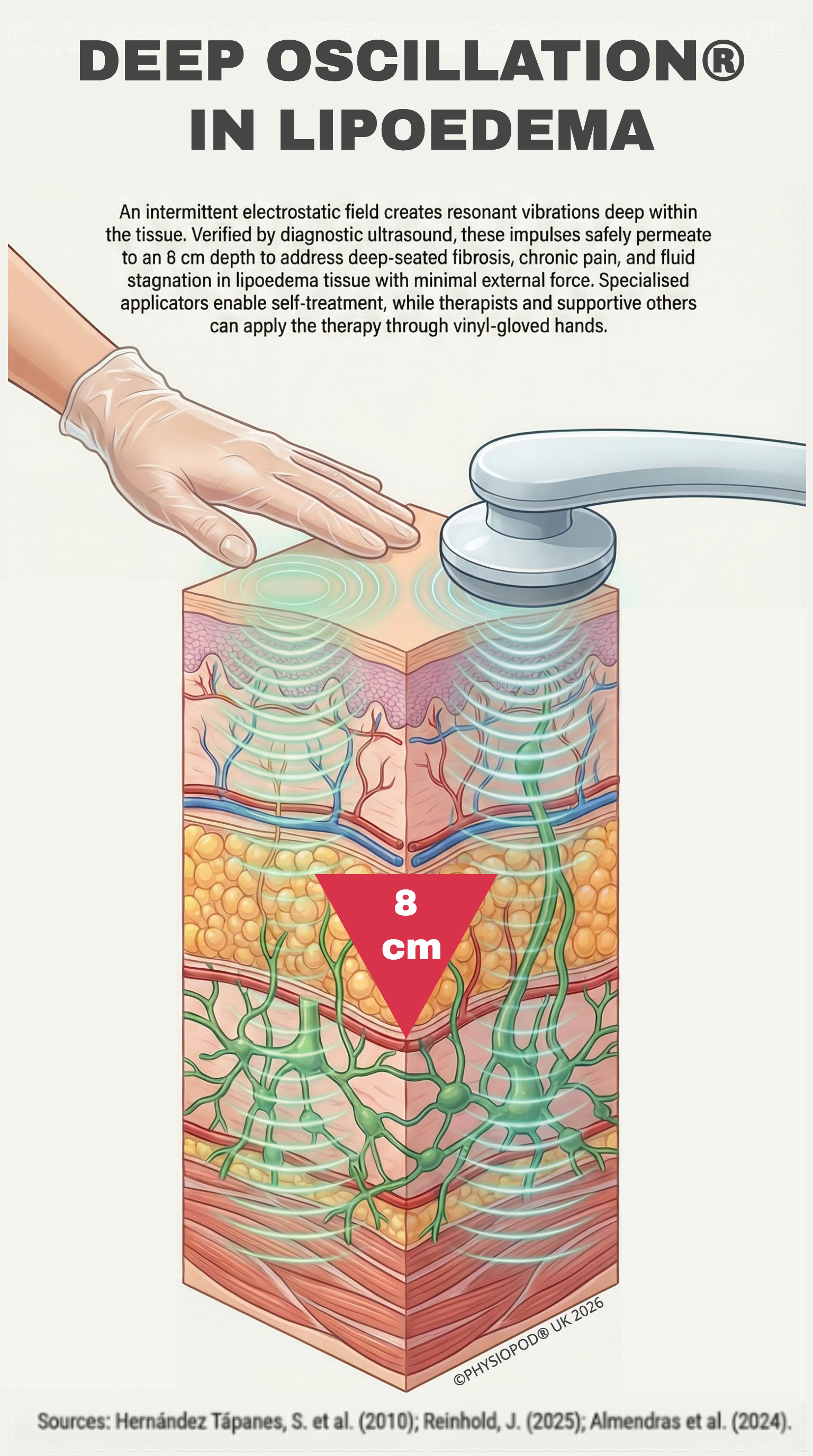
Figure 3: Deep Oscillation® in Lipoedema. An intermittent electrostatic field creates resonant vibrations deep within the tissue. Verified by diagnostic ultrasound, these impulses safely permeate to an 8 cm depth to address deep-seated fibrosis, chronic pain, and fluid stagnation in lipoedema tissue with minimal external force. Specialised applicators enable self-treatment, while therapists and supportive others can apply the therapy through vinyl-gloved hands. Crucially, unlike conventional electrotherapy, which acts primarily on the neuromuscular system, Deep Oscillation intervenes directly in the connective tissue—making it specifically effective for addressing the structural fibrosis and pathological adipose changes characteristic of lipoedema. Clinical verification of the 8 cm penetration depth via diagnostic ultrasound provided by Dr. Solangel Hernández Tápanes (2010).
© Copyright 2026 PhysioPod® UK Ltd.
Unlike traditional mechanical therapies or massages that rely on physical pressure—which can be agonising for hypersensitive lipoedema tissue—Deep Oscillation operates on a completely different, externally applied principle. According to expert consensus (Reinhold, 2025), the therapy utilises an intermittent electrostatic field created between the device applicator and the patient's tissue to generate a gentle, biologically effective vibration (oscillation).
Importantly, diagnostic ultrasound studies demonstrate that this non-traumatic oscillation can penetrate up to 8 cm depth. A clinical study by Hernández Tápanes et al. (2010) visually verified that these impulses penetrate through the skin, connective tissue, and subcutaneous fat, and extend into the muscles. This 8 cm depth suggests the therapy can effectively target the diseased connective adipose tissue without applying painful external force. A 2024 literature review by Almendras et al. reports the efficacy of these deep oscillations for lipoedema, suggesting powerful anti-fibrotic and anti-oedema effects.
Furthermore, the clinical utility of Deep Oscillation in treating hard-to-massage, deep-seated fibrosis has been reported in observational studies using the internationally recognised Glasgow Benefit Inventory (GBI) (Halliday et al., 2020), while robust evidence from a randomized controlled clinical trial on comparable fibrotic connective tissue models demonstrates that Deep Oscillation effectively reduces both pain and deep tissue induration (Hernández Tápanes et al., 2018).
Furthermore, a forthcoming 2026 service evaluation by Fickling highlights that Deep Oscillation provides a distinct clinical advantage: it successfully softens hard, deep-tissue induration (the "fibrosis gap") while simultaneously reducing the physical strain and workload on an overstretched clinical workforce.
Biochemical Pain Relief and Frequency Targeting: Deep Oscillation provides highly customisable treatment through specific frequency ranges. High frequencies (80–250 Hz) are typically used initially to dissolve tissue hardening and reduce pain; medium frequencies (25–80 Hz) induce muscle relaxation and stimulate fluid flow; and low frequencies (5–25 Hz) generate a powerful pumping effect to promote venous and lymphatic drainage (Kraus, Lymphologischer Informationsdienst). Evidence suggests that by improving microcirculation and metabolic exchange at this deep cellular level, the therapy helps flush out pain-transmitting substances such as serotonin, bradykinin, and prostaglandins, directly addressing the chronic pain syndromes and tissue induration associated with conditions like lipoedema, resulting in consecutive improved mobility (Hernández Tápanes et al., 2018)
Application Methods: Device Applicators and Vinyl-Gloved Hands
Deep Oscillation therapy offers highly versatile methods of application to suit both professional clinical settings and daily home care. The therapy can be administered directly using special hand-held device applicators, which generate the intermittent electrostatic field between the applicator and the patient's tissue (Reinhold, 2025). These applicators are particularly advantageous for patients performing independent self-management at home, empowering them to effectively target deep tissue fibrosis, pain, and fluid stagnation using targeted dual-applicators on the affected limbs.
In a professional clinical setting, however, the therapy can be applied directly through the therapist's hands. By wearing vinyl gloves, the Manual Lymphatic Drainage (MLD) practitioner acts as the physical conduit for the electrostatic field. This innovative application allows the therapist to deliver a highly effective, deep-tissue treatment using significantly gentler manual pressure (Reinhold, 2025; Almendras et al., 2024). Because lipoedema is often characterised by sensitive, "fibro-fatty" tissue, achieving deep tissue release using firm manual pressure alone can be highly uncomfortable for patients and physically exhausting for the therapist. By using gloved hands, the electrostatic field powerfully enhances the practitioner's manual techniques. It reduces the biomechanical strain required to mobilise fibrotic tissue, preventing physical exhaustion and allowing therapists to work more efficiently with less fatigue (Fickling, 2026).
Video 1: The Clinical Appeal of Deep Oscillation Therapy. A visual demonstration of therapists applying the treatment to create gentle, biologically effective oscillations. Watch how the therapy safely penetrates up to 8 cm deep to target connective tissue, fat, and lymph vessels for both conservative and post-surgical lipoedema management.
Manual Lymphatic Drainage (MLD) is widely recognised by specialists as a cornerstone therapy for managing lipoedema and supporting patients who develop secondary lipo-lymphoedema. As a highly specialised, hands-on therapy, MLD stimulates the lymphatic system and helps move excess fluid away from congested areas. However, because lipoedema is often characterised by deep-seated "fibro-fatty" tissue, achieving deep tissue release using firm manual pressure alone can be physically exhausting for the therapist, and uncomfortable for those patients who experience tissue tenderness.
To address these challenges, expert consensus and literature reviews suggest that advanced adjunctive therapies like Deep Oscillation can serve as a valuable extension of the MLD practitioner's capabilities (Reinhold, 2025; Almendras et al., 2024). By wearing vinyl gloves, the therapist acts as the conduit for the electrostatic field, which has been reported to deliver deep-tissue treatment using significantly gentler manual pressure. The efficacy of this combined approach has been documented across multiple levels of evidence; service evaluations in Wounds International highlight the successful integration of Deep Oscillation with MLD in the management of lower-limb lipoedema (Teo, Coulborn, & Munnoch, 2018), while retrospective case studies similarly report that incorporating Deep Oscillation into standard MLD protocols yields significant symptom and fluid reduction (Nourollahi et al., 2013).Clinical observations suggest that this combined approach allows therapists to simultaneously target compromised lymph vessels and reduce local congestion.
Furthermore, a forthcoming 2026 UK independent service evaluation by Fickling reports that practitioners observe "significant softening" of deep tissue, noting that the therapy "acts deeper than possible with manual therapy." According to this evaluation, integrating the device may yield "quicker improvements" than MLD alone, offering a potential efficiency dividend for clinics facing staffing restrictions. Practitioners within the service evaluation reported that Deep Oscillation delivers greater "time efficiency" and "frees up clinic slots," while also reducing the biomechanical strain on the workforce, with therapists explicitly reporting "less workload" and less fatigue (Fickling, 2026).
Aligning with the 2026 Delphi Consensus
While the 2026 Delphi Consensus does not endorse specific commercial device brands, Statement 41 validates that lipoedema pain and physical sensitivity can be effectively reduced by "complete physical decongestive therapy or other physical therapies" (Kruppa et al., 2026). The evidence suggests that Deep Oscillation aligns well with this global mandate. By integrating this modality, service evaluations and retrospective data indicate that MLD therapists can utilise an evidence-based adjunct to elevate their standard of care and effectively support patient outcomes.
While the UK's National Institute for Health and Care Excellence previously advised that liposuction be used only in a research setting (NICE, 2022), 2026 marks the era of evidence-based lipoedema care challenging this paradigm. The groundbreaking German LIPLEG study and the 2026 Lipedema World Alliance Delphi Consensus have officially validated lymph-sparing liposuction (such as Water-Assisted and Power-Assisted Liposuction) as a medically necessary treatment to remove diseased tissue and significantly alleviate pain when conservative therapies fall short (Podda et al., 2021; Seefeldt et al., 2023).
However, the European Lipedema Forum and recent 2026 surgical guidelines stress the importance of strict patient selection to ensure safety and efficacy. Liposuction is generally recommended for patients who have undergone at least 6 months of conservative therapy without symptom resolution, and who maintain a BMI of 35 kg/m² or lower, with careful consideration required for those exhibiting central obesity (a Waist-to-Height Ratio > 0.5).
To optimise these advanced procedures, international surgical consensus strongly advocates for integrating adjunctive therapies. Specialist surgeons—such as leading UK Consultant Plastic Surgeon Mr Vasu Karri—highly recommend Deep Oscillation to prepare the tissue pre-operatively. This protocol is further echoed in comprehensive clinical guides, such as 'All About Lipedema' authored by leading German specialist Dr. Dominik von Lukowicz and colleagues, which prominently features Deep Oscillation as a core treatment modality (von Lukowicz et al., 2021). Clinical experience shows that the therapy effectively softens deep fibrosis, resulting in less bleeding, fewer complications, and a quicker recovery. Because of its gentle, non-invasive nature, it can be safely applied from day one post-operatively to accelerate the wound-healing process, inhibit local inflammation, and significantly reduce pain, bruising and swelling.
As of 2026, the introduction of Glucagon-like peptide-1 (GLP-1) and dual GIP/GLP-1 receptor agonists (such as semaglutide, tirzepatide, and exenatide) has opened a new frontier in the conservative management of lipoedema. While clinical consensus explicitly states that there are currently no pharmacological interventions that can "cure" or selectively dissolve established fibrotic lipoedema tissue, these medications are showing significant promise as disease-modifying therapies.
Recent clinical data highlights that GLP-1 agonists can successfully target the systemic inflammation, insulin resistance, and macrophage-driven pathways inherent to the disease. For example, an Italian pilot study evaluating exenatide in women with lipoedema and insulin resistance reported a reduction in pain evoked by pinching the tissue fold, as well as a decrease in subcutaneous fat thickness, suggesting the medication helped break the cycle of inflammation. Furthermore, recent reviews highlight tirzepatide—a dual GLP-1/GIP agonist—as a potential disease-modifying therapy that can simultaneously address metabolic, inflammatory, and fibrotic pathways to restore adipose tissue flexibility.
For patients with coincident secondary obesity, these medications serve as a powerful adjunctive tool to remove "regular" metabolic fat. By facilitating the loss of this standard fat, GLP-1 agonists help decompress the lymphatic system (potentially improving flow and reducing swelling), reduce the weight-bearing strain on joints, and improve overall mobility. Because these medications actively influence immune signalling and fat tissue health, clinical experts emphasise that a "low and slow" dosing approach is particularly relevant for the lipoedema population to safely manage the metabolic shift.
Ultimately, researchers emphasise that GLP-1 agonists are not a standalone cure and must be integrated into a multimodal protocol where conservative treatment, exercise, and diet remain paramount (Faria et al., 2026). Within this comprehensive framework, advanced physical therapies like Deep Oscillation remain perfectly positioned to actively soften the localised, deep-tissue induration that medications alone cannot resolve.
If you are struggling to get your GP to recognise your symptoms, you are not alone. Because lipoedema is frequently misdiagnosed as standard obesity or lymphoedema, you may need to help guide your doctor. Here is an evidence-based, UK-specific "toolkit" you can take to your next appointment:
- Shift the Focus from Fluid to Tissue Texture: If your GP focuses solely on fluid swelling (oedema), gently explain that lipoedema is primarily a connective tissue disorder, meaning the fat itself is physically altered. While many women experience varying degrees of pain, heaviness, or tenderness, the intensity varies from person to person. Regardless of your specific pain levels, ask your GP to physically feel the skin for the condition's characteristic nodular, "granular," or pebbly texture, rather than just looking for fluid retention.
- The RCGP eLearning Course: Inform your doctor that the Royal College of General Practitioners (RCGP), in partnership with the charity Lipoedema UK, has a dedicated eLearning course specifically on diagnosing lipoedema.
- Take the Lipoedema UK "How to Recognise" Leaflet: Download and print Lipoedema UK's specific "How to recognise" leaflet directly from their website to bring along to your appointment. This is an excellent visual tool to help guide your GP through your symptoms.
- UK Best Practice Guidelines: Print out and hand them the UK Best Practice Guidelines: The Management of Lipoedema (published by Wounds UK), which clearly outlines the condition and is widely recognised by UK practitioners.
- Ask for Specific Clinical Tests: Ask your GP to physically check for the "cuffing sign" at your ankles or wrists (where the fat stops abruptly, leaving the hands and feet "spared") and to look for the characteristic fat pads on the inner sides of your knees.
- Explain the "Stemmer's Sign" for Differential Diagnosis: While your feet may visually appear "spared" (unaffected by the disproportionate tissue in your legs), ask your doctor to physically confirm this by checking for a "Stemmer's sign" on your toes. You may need to explain that this means trying to pinch or pick up a fold of skin at the base of the second toe. Because standard lymphoedema usually involves the feet, demonstrating a negative Stemmer's sign (meaning the doctor can easily pinch the skin) is a vital clinical step to definitively distinguish lipoedema from standard lymphoedema (Kruppa et al., 2026)
- Challenge the BMI and Clarify the Diagnosis: If your GP focuses solely on your weight, share the latest 2026 medical consensus: BMI is officially recognised as a flawed and misleading metric for lipoedema because the heavy, pathological fat in the limbs artificially inflates the reading (Luta et al., 2025; Kruppa et al., 2026). It is vital to help your GP distinguish between these frequently confused conditions: unlike generalised obesity (which is proportionate, affects the whole body, and responds to calorie deficits) or lymphoedema (a fluid-driven, often asymmetrical swelling that typically involves the feet), lipoedema is a distinct, nodular connective tissue disease that uniquely spares the hands and feet. Ask your GP to assess your true metabolic health using the Waist-to-Height Ratio (WHtR) instead, as this is the clinically validated method to differentiate truncal obesity from lipoedema-specific limb volume (Brenner et al., 2023; Kruppa et al., 2026; Luta et al., 2025).
5.0 Finding Expert Care & Support
Navigating the healthcare system with lipoedema can feel isolating, but there is a robust network of professional care and charitable support available across the UK, Northern Ireland, and the Republic of Ireland.
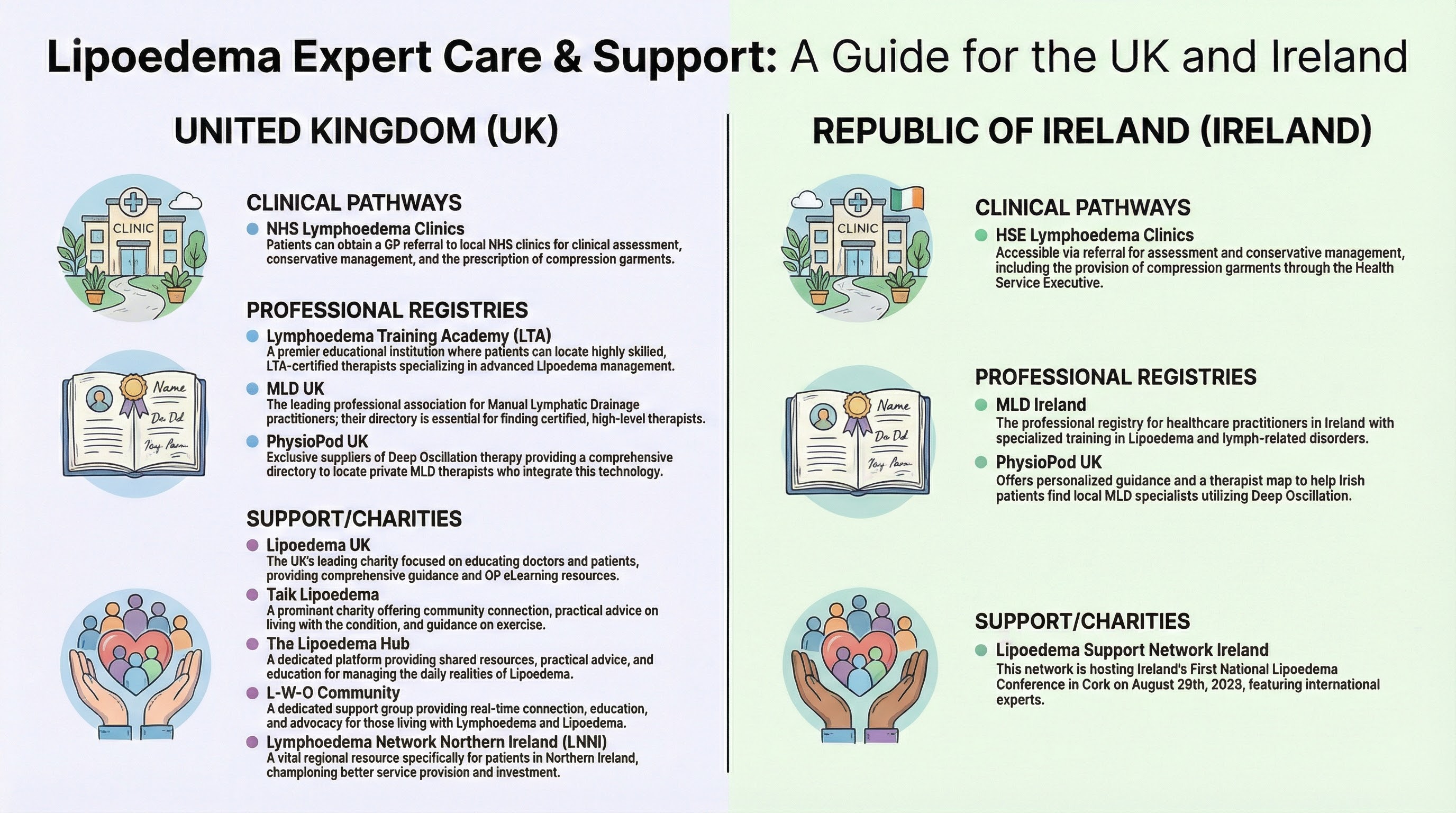
Figure 4: Finding Expert Care and Support for Lipoedema. A comprehensive UK & Ireland roadmap guiding patients through private specialist care, NHS/HSE clinical pathways, and dedicated patient charities and support networks. Full links in section 11.0 Useful Resources & Further Reading
© Copyright 2026 PhysioPod® UK Ltd.
If you are looking to experience the specific benefits of Deep Oscillation Therapy, PhysioPod® UK provides a comprehensive directory. As the exclusive suppliers for Deep Oscillation across the UK and Ireland, the PhysioPod team can help you connect with local experts.
Professional Expertise: You can locate highly qualified private Manual Lymphatic Drainage (MLD) therapists across the UK and Ireland who integrate Deep Oscillation into their practice.
Specialist Recommendations: If you have secondary lymphoedema or are preparing for lipoedema liposuction, PhysioPod® specifically recommends seeking out a fully certified private MLD DLT Lymphoedema therapist.
Personalised Guidance: If you are unsure which therapist is right for you, you can provide your postcode to the PhysioPod® team, and they will help you find a local specialist.
Lymphoedema Training Academy (LTA): A premier educational institution providing advanced, highly specialist training in lipoedema and lymphoedema management. Their professional network is an excellent, trusted way for patients to find rigorously skilled, LTA-certified therapists near them.
MLD UK: The leading professional association for Manual Lymphatic Drainage practitioners in the UK. Their directory serves as an essential, highly respected resource for finding comprehensively trained and fully certified therapists dedicated to lymphatic health.
MLD Ireland: The dedicated professional organisation of healthcare practitioners in the Republic of Ireland who have obtained advanced, specialised training to provide expert treatment in the management of lipoedema and lymph-related disorders. Their register is a vital resource for connecting with highly skilled local therapists.
Lymphoedema Network Northern Ireland (LNNI): A vital and proactive resource for patients in Northern Ireland, LNNI continuously champions better clinical service provision, essential patient education, and increased investment in lymphatic care.
NHS / HSE Lymphoedema Clinics: While subject to regional availability, your GP can refer you to your local NHS (UK) or HSE (Ireland) Lymphoedema service for a formal assessment, conservative management planning, and the prescription of compression garments.
Connecting with dedicated support platforms is one of the most important steps a patient can take for education, emotional support, and self-advocacy.
Lipoedema UK: The UK's leading charity dedicated to educating doctors and patients. As a founding member of the Lipoedema World Alliance, they provide comprehensive guidance, support the RCGP eLearning course for GPs, and host vital patient and healthcare support resources. Lipoedema UK also host regular member webinars featuring presentations from highly prestigious international experts.
Talk Lipoedema: A prominent charity offering vital community connection, emotional support, and highly practical advice on living with the condition. They are a leading resource for daily self-management, providing the community with dedicated guidance, visual tools, and evidence-based strategies for exercise, self-lymphatic drainage, and dry skin brushing.
Lipoedema Hub: Founded by Bel Hardman based on her own lived experience with the condition, this is a free, community-driven directory designed to connect patients with trusted therapists, supportive practitioners, and helpful products. By bringing scattered knowledge into one central, accessible place, the Hub bridges clinical expertise with real patient insight. Its mission is to remove barriers and eliminate the frustrating, lengthy search for care, making it significantly easier for women to find diagnosis pathways and compassionate, informed support.
L-W-O Community: A dedicated patient support group providing real-time community connection, education, and advocacy for those living with lymphoedema and lipoedema. They are highly proactive in patient-led research and awareness, having collaborated extensively on World Lymphoedema Day campaigns and community surveys focusing on the vital benefits of deep breathing and Self-Lymphatic Drainage (SLD).
Lipoedema Support Network Ireland: A dedicated patient support group offering vital connection and advocacy for the Republic of Ireland. In a significant milestone for the Irish lipoedema community, they are proud hosts of the 2026 National Lipoedema Conference, scheduled for Saturday, 29th August 2026, at the Cork International Hotel. Led clinically by Prof. Dr. med. Mojtaba Ghods, the event will bring together patients, MLD therapists, and international experts. The PhysioPod® team will also be exhibiting at the event to showcase how DEEP OSCILLATION® can enhance daily lipoedema care at home.
6.0 Take Control at Home: The Deep Oscillation Personal Basic - Because lipoedema, is a chronic condition, long-term self-management is vital.

Figure 5: Independent Lipoedema Management with Deep Oscillation. A patient demonstrating self-treatment using the Deep Oscillation Personal Basic unit with dual applicators on the lower limb, permeating 8cm depth and making treatment time effective. This non-invasive, home-based therapy allows individuals to effectively manage daily symptoms such as pain, swelling, bruising and deep tissue fibrosis, helping to reduce the feeling of heavy limbs. © Copyright 2026 PhysioPod® UK Ltd
Regional healthcare pathways, including the latest lipoedema guidelines published by NHS Wales, explicitly recommend the use of hand-held massagers to stimulate circulation, improve tissue oxygenation, and reduce inflammation (Lymphoedema Wales Clinical Network, 2025).
For those who need to manage these symptoms daily, purchasing a Deep Oscillation Personal Basic unit provides the ultimate home solution. This device is a "game-changer" for independent care, offering several key advantages:
- Clinical Strength: The Basic unit is just as powerful as the professional models used by clinicians.
- Conservative Management: It effectively targets pain, bruising, swelling, inflammation, and fibrosis.
- Bespoke Therapy: Each unit includes a special therapy card from PhysioPod® designed specifically for lipoedema based on 16 years of experience.
- Pre- and Post-Surgery Support: Recommended by leading specialist surgeon Mr Vasu Karri in the UK, Deep Oscillation softens fat before surgery and accelerates healing from the very early post-operative stage.
Expert Support Every Step of the Way
Investing in a personal unit is not just a purchase; it’s a partnership with PhysioPod® UK. When you buy a unit, you receive a one-to-one Zoom setup session with Julie to ensure you are confident in your self-treatment. For those not ready to buy, short-term surgical recovery options are also available.
Clinical consensus within UK community nursing highlights that early detection and a multimodal approach—combining specialist treatments with dedicated self-management—are key to preventing lipoedema progression (Fetzer, 2016). While professional interventions and surgical care are critical, daily self-management empowers patients to actively control their symptoms. Alongside home-use devices like the Deep Oscillation® Personal Basic, integrating the following evidence-based conservative tools into a daily routine can significantly improve quality of life and enhance the effects of clinical treatments:
• Flat-Knitted Compression Therapy: The clinical gold standard for lipoedema management. Unlike standard circular-knit garments, Class 2 (or higher) flat-knitted garments are structurally designed to stabilise limb volume, resist rolling or cutting into sensitive fibrotic tissue, and provide a continuous "micro-massage" effect during movement (Czerwinska et al., 2023; Wright et al., 2023).
• Targeted Nutritional Support: Under medical guidance, specific supplements can address the chronic inflammation and microcirculation issues inherent in lipoedema. Clinical trials have demonstrated that Pycnogenol® (a potent plant-based antioxidant) can help progressively reduce symptom severity (Netto et al., 2025), while minerals like Selenium assist in negatively regulating inflammatory markers and addressing deficiencies within adipose tissue (Nourollahi et al., 2013; Pfister et al., 2020).
• Intermittent Pneumatic Compression (IPC): Intermittent Pneumatic Compression (IPC) is a widely recognised adjunctive therapy in the UK for the conservative management of lipoedema. IPC devices utilise cyclical inflatable garments to mechanically stimulate lymphatic flow, which helps prevent fluid accumulation and alleviate debilitating symptoms such as tissue inflammation and pain. A comprehensive review of specialist approaches in the British Journal of Community Nursing identifies IPC as one of the most common treatments for lipoedema, noting that when integrated early and appropriately into a self-care routine, it can provide huge benefits for patients managing the condition at home.
• Hydrostatic and Low-Impact Movement: Because lipoedema is frequently accompanied by joint hypermobility, high-impact exercise can be damaging. Aquatic therapy and hydrostatic low-impact movements—such as aquacycling and swimming—are highly recommended. Swimming is particularly valuable as it is universally accessible, and the water provides natural hydrostatic compression while completely removing the heavy, painful gravitational strain from the joints (Burger et al., 2019)
• Superficial Lymphatic Stimulation: Kinesiology taping (Michelini et al., 2023) can microscopically lift the skin to stimulate the superficial lymphatic capillaries, aiding daily fluid movement between professional MLD sessions.
• Targeted Skin Care and Oxygenation: Due to stagnant lymphatic flow and compromised microcirculation, lipoedema tissue frequently suffers from reduced oxygenation and impaired metabolic exchange. Regional clinical networks explicitly recommend mechanical and lymphatic stimulation—such as the use of hand-held massagers or targeted massage—to improve tissue oxygenation, facilitate nutrient delivery, and protect the integrity of the skin barrier. Devices like the Deep Oscillation Personal Basic directly fulfill this clinical mandate by providing an advanced, non-invasive method to stimulate microcirculation and support daily skin health (Kraus; Reinhold, 2025)
7. Conclusion & Special Acknowledgements
The year 2026 marks a watershed moment in the clinical recognition and evidence-based management of lipoedema. With the WHO's global recognition under the ICD-11 classification, the establishment of highly specific 2026 ICD-10-CM diagnostic codes, the publication of the Lipedema World Alliance Delphi Consensus, and the clinical validation that this pathological tissue is resistant to traditional diets, the narrative has fundamentally shifted. Lipoedema is no longer an unrecognised or untreatable condition; it is a disease that is comprehensively managed. Reclaiming your quality of life requires a proactive, multimodal approach:
- Advocate for an Accurate Diagnosis: Utilise your GP Toolkit and request that your condition is formally assessed using the Waist-to-Height Ratio (WHtR) rather than BMI alone, and ensure your diagnosis is officially documented using the appropriate codes (such as the global WHO ICD-11 code EF02.2 or the newly updated 2026 ICD-10-CM E88.2 series).
- Optimise Conservative Management: Integrate advanced adjunctive therapies like Deep Oscillation alongside MLD and flat-knitted compression to proactively target pain, preserve lymphatic function, and soften deep tissue fibrosis.
- Embrace Targeted Nutrition and Pharmacotherapy: Work with specialists to explore intensive anti-inflammatory lifestyle changes (such as ketogenic or low-carbohydrate diets) and discuss the emerging role of GLP-1 agonists or antioxidant supplements to manage systemic inflammation and metabolic burden.
- Explore Evidence-Based Surgical Options: If conservative measures fall short, consult with a UK specialist regarding lymph-sparing liposuction. Ensure you meet the latest patient selection criteria and plan for day-one/early post-operative Deep Oscillation therapy to accelerate your recovery and reduce bruising.
- Prioritise Emotional Well-being: Clinical consensus emphasises that lipoedema management must be a multimodal, holistic approach rather than just a physical one. Patients frequently endure years of misdiagnosis, ineffective traditional calorie restriction, and clinical advice based solely on BMI. This historical lack of recognition contributes heavily to the disease's psychosocial burden, driving a high prevalence of anxiety, depression, and distress. It is essential to set realistic long-term treatment expectations with your physician, validate your lived experiences, and actively address this psychological and emotional toll (Forner-Cordero et al., 2021, Luta et al., 2025).
Because lipoedema affects multiple biological systems—spanning systemic inflammation, lymphatic congestion, and deep-tissue fibrosis—no single therapy can act as a standalone cure. Specialists emphasise that successful management absolutely requires a "team effort" via a multimodal protocol, combining pharmacological agents, physiotherapy, mechanical strategies, and potential surgical interventions to target every layer of the pathology.
By taking these strategic steps today, you are laying the foundation for a transformative year. Imagine where you could be by the end of 2026: experiencing significantly less pain, regaining the mobility to participate in activities you have long avoided, and feeling confident and empowered with the knowledge and tools for long-term, independent management. Your journey to reclaiming your health starts with a single, informed step.
Special Acknowledgements
PhysioPod® UK would like to extend our deepest gratitude to the following individuals and organisations. Your invaluable contributions, clinical reviews, and shared wisdom were instrumental in shaping this 2026 Review into a comprehensive, accurate, and truly readable document:
- Jane Wigg (Lymphoedema Training Academy - LTA): For your amazing "24/7" dedication, unending support, eagle eye and outstanding commitment to advancing lymphatic education and care.
- Catherine Groom: Specialist Lymphoedema Practitioner, for your clinical expertise, meticulous reading, and vital contributions to the practical guidance within this document.
- The Team at Lipoedema Support Network Ireland (LSNI): For your incredible advocacy and for generously sharing your brilliant, accessible summaries from the 2025 Lipoedema World Congress.
- Jacqueline (Jax) Smith: Patient advocate, regular PhysioPod guest blogger, and lipo-lymphoedema warrior. Your powerful insights into the lived reality of the condition—from the physiological toll of chronic pain to the importance of skin oxygenation—ensured the patient voice remained at the very heart of this review.
This article was written with the assistance of AI to review, combine, and organise information. AI was utilised to translate complex clinical data—and the tissue-level effects of Deep Oscillation—into an accessible format to empower patients and assist doctors. While AI helped structure the article and develop the 'GP Toolkit', all clinical facts, terminology, and treatment effectiveness data come directly from the research and guidelines published by the cited medical experts. This AI-assisted summary is intended for educational and informational purposes only and should not be used as a substitute for a professional consultation with a qualified medical professional.
9. Keywords & Glossary of Clinical Terms
Keywords: Lipoedema, Lipedema, Lipalgia Syndrome, Deep Oscillation Therapy, Lipedema World Alliance Delphi Consensus, Lymph-Sparing Liposuction, Multi-omics, Waist-to-Height Ratio (WHtR), ICD-11, ICD-10-CM 2026, Negative Stemmer's Sign, Mast Cells, MicroRNAs, GLP-1 Agonists.
Glossary of Clinical Terms:
- Artificial Intelligence (AI): Used in the context of this article strictly to assist in the review, translation, and structuring of complex clinical data and physiological research into an accessible, educational format for patients and doctors.
- Complex Decongestive Therapy (CDT): The standard conservative management approach for lymphatic and adipose disorders. It typically includes a combination of manual lymphatic drainage (MLD), compression garments, skin care, and exercise.
- Deep Oscillation Therapy (DOT): An advanced non-invasive therapy utilising electrostatic impulses to create resonant vibrations that penetrate up to 8 cm deep into tissue. It is clinically used to soften deep-seated fibrosis, reduce pain, and enhance lymphatic drainage.
- Fibro-fatty Scarring (Fibrosis): The pathological thickening, hardening, and scarring of connective tissue. In lipoedema, this creates the painful, "nodular", or "woody" texture that acts as a mechanical barrier to fluid drainage.
- GLP-1 Agonists: A class of medications that help manage systemic inflammation and metabolic burden. Because they actively influence immune signalling, clinical experts recommend a "low and slow" dosing approach for lipoedema patients.
- ICD-11 & ICD-10-CM 2026: The official medical diagnostic coding systems used globally. The WHO's ICD-11 classifies lipoedema under code EF02.2. The newly updated 2026 ICD-10-CM introduces highly specific codes for lipoedema stages (E88.21 for Stage 1, E88.22 for Stage 2, and E88.23 for Stage 3).
- Lipalgia Syndrome: A regional administrative term used by some NHS trusts (such as Lymphoedema Wales and LNNI) as an alternative name for lipoedema (Lymphoedema Wales Clinical Network, 2025; LNNI, 2025). Translating to "painful fat," the term was locally introduced to help distinguish the condition from fluid-driven lymphoedema. However, this terminology is highly contested; the 2026 global consensus officially confirms that pain intensity varies widely, meaning many patients do not experience the severe tissue tenderness the name implies. Because of this, "lipoedema" remains the globally recognised standard.
- Lipedema World Alliance (LWA) Delphi Consensus: A landmark 2026 international agreement published in Nature Communications, which established 59 expert consensus statements standardising the diagnosis, pathophysiology, and management of lipoedema globally.
- Macrophage Polarisation: The process where immune cells (macrophages) change their behaviour. In lipoedema tissue, an abnormal predominance of "M2" macrophages is believed to drive chronic tissue inflammation and abnormal fat expansion.
- Mast Cells: Immune cells that, when overactive within lipoedema tissue, are now understood to significantly contribute to the condition's characteristic pain, swelling, and chronic immune activation.
- MicroRNAs: Small molecules that regulate gene expression. In lipoedema, changes in microRNAs and altered stem-cell behaviour disrupt normal genetic regulation, fundamentally contributing to the abnormal expansion of fat.
- Multi-omics: A cutting-edge biological research approach that looks at multiple data sets at once (such as genetics, proteins, and metabolism) to identify the underlying disease mechanisms and molecular hallmarks of lipoedema.
- Negative Kaposi-Stemmer's Sign: A physical clinical test. If a doctor can pinch and lift a fold of skin at the base of the second toe, the test is "negative." A negative sign combined with heavy, painful legs strongly indicates lipoedema rather than standard lymphoedema.
- Waist-to-Height Ratio (WHtR): A measurement used to assess metabolic health. The 2026 Delphi Consensus confirms WHtR is much more accurate than the Body Mass Index (BMI) for lipoedema patients, as it accounts for the disproportionate fat carried on the lower body without automatically categorising the patient as obese.
