Caesarean Section Scar Analysis & Treatment Plan - THE SCAR BEYOND
from Christine Talbot, Lymphoedema and Bowen Practitioner

In January 2021, PhysioPod had been contacted by a young lady in the East of England who was desperately researching/seeking reasons and treatment solutions to the intense musculoskeletal and nerve pain following her caesarean section nine months previously. At four months postpartum, Mrs M was getting back to normal taking her young girls out and so on, but suddenly, in September 2020 at five months post caesarean-section, she experienced a sudden sharp electrical shooting pain from the right hip area at the top right-hand side of the incision, down through the rectus abdominals down into the groin and genitalia. This whole sensation reoccurred frequently, becoming persistent in nature as nerve pain. It settled a little but left an electrical sensation, she then experienced a persistent medial pain into her left foot, this foot remains weak, with a loss of muscle tone. Quite possibly as pre-pregnancy hormones returned to normal, muscular tonicity changed and tightened causing severe pain due to structural non-alignment.
Her Obstetrician deemed every thing 'normal' from their perspective, she received a Caesarean Section Massage. Mrs M made many calls to her GP and visited A&E on three plus occasions, such was the intolerable pain. Various tests and scans were carried out but she did not receive the pelvic MRI results. Mrs M self-funded two Osteopaths and a Chiropractor to ascertain and diagnose her increasing right sided pain and tightness, radiating deep into her right groin, perineum, into her back and down her right leg, this right-sided tightness and intense nerve pain was in contrast to the flaccid looseness throughout the whole of her left side. The scar was considered to be hypertrophic with suboptimal healing, it was being suggested she had Osteitis Pubis. A traumatised Amygdala and learnt pain. An inguinal hernia was also suggested, though I felt that it was is unlikely that this would cause such structural change and disability in a young person. A final suggestion was made of carrying out lower back surgery for a compressed or trapped nerve, however, a recent MRI did not show any nerve entrapment or compression.
In late January 2021, with the young lady's permission, Mary forwarded a current photograph of the abdo-pelvic post caesarean scar. I was informed the young lady was hiring a Deep Oscillation Personal unit and a Magcell and would I guide her through the use of the machines?
Background History
Mrs M experienced a very traumatic birth with her first child, the memories of which ultimately dictated the outcome of the birth with her second child. The birth in April 2020 coincided during the first Covid lockdown when strict restrictions were in place throughout the country and in particular, hospitals had a no visitor policy. Expectant Mothers were allowed little or no support from their partners during labour. Mrs M was very conflicted at this point as to whether to proceed with a normal labour, which was her birthing choice or to opt for a caesarean, a friend had suggested this option to her, as she was very anxious in light of her previous experience. A midwife informed her mothers were booking caesarean sections right left and centre to beat a staffing crisis, Mrs M noticed staff were very anxious as this was the first time they were in full PPE with the whole Covid situation escalating at an alarming rate.
Mrs M contacted me shortly after I received Picture 1. from Mary We talked at great length on the phone, I was shocked to hear of the neglect she had received regarding her first birthing experience, these are precious moments that can never be undone or regained in a nurturing compassionate magical memory and inevitably have a lasting effect. I was equally concerned by her intense feeling of guilt and failure towards her family and herself, at having been seemingly coerced into a caesarean section and wondered whether the scar manifestation was indicative of a double trauma in a physical presentation. I asked whether Mrs M had ever fallen on her coccyx, she used to ride horses and had many such falls and injuries, these silent youthful injuries can have a profound effect later in life.

Picture 1. Shows a raised reddened scar deviating diagonally upwards towards the right hip, there is a marked lumpiness around the scar and above the right side there is a darkened discolouration which Mrs M said was very painful.

Picture 2. Shows a remarkable difference in the appearance of the scar after just one session with deep oscillation, although the scar looks calmer and less reddened there remains a diagonal pull upwards on the right and a noticeable tightness of the right hip flexor in contrast to the left.
It was evident from Pic 2. that the scar responded very favourably to the first treatment of deep oscillation, the reddened lumpiness was significantly less, the scar was more moveable and less distressed in appearance. I had instructed Mrs M in how to move the applicator head over the area to aid mobilisation of the skin and to oil the scar with Argan or Rose Hip oil to soften and feed the scar with vitamins in the oil. Clearly the localised treatment was effective, enhanced by the Magcell to aid blood supply to the scar and surrounding tissue. However, the darkened, bruised area superior and diagonally lateral to the scar was unchanged so too, the tightness in the right iliac fossa with little relief from the muscular skeletal nerve related pain. Initially, I thought the darkened area might be an unresolved haematoma but I gather the Osteopath had gone deep into the hip related areas to gain some relief to the sciatic nerve, so this may have caused internal bruising.
I spoke with 'Mrs M every week over the phone guiding her as to how best to use the equipment loaned to her through PhysioPod, which she was using diligently making great progress with scar management. All this she was doing as a mother of two very young children, whilst alone trying desperately to get answers to her genuine physiological post pregnancy and operative delivery change. I suggested small incremental exercises to initiate nerve and muscle memory. I felt too, it was essential to remain in very regular contact with Mrs M as her anxiety levels were understandably very high and there was a significant danger of increasing depression through what Mrs M had felt was 'professional abandonment and isolation'. She needed someone on whom to off load and someone who understood the probable origins of her clinical presentation.

Picture 3. Scar line fading, hip appears to be higher on the right.
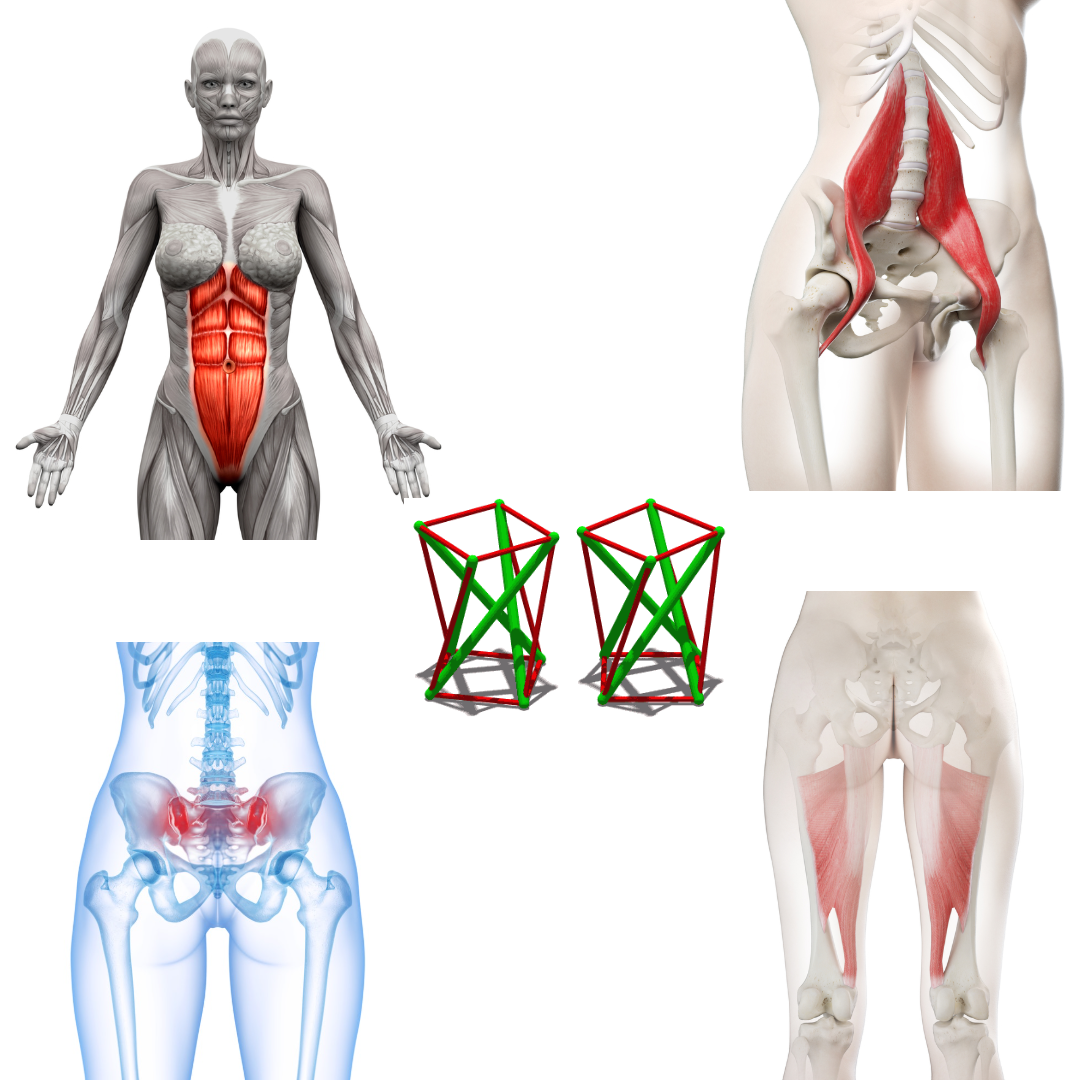
As an adjunct to deep oscillation and Magcell therapy, Mrs M bought a low-level laser to assist with scar work and other painful areas around the sacrum and perineum. At one point I was concerned Mrs M might have Complex Regional Pain Syndrome (CRPS) as nothing was resolving. She told me she felt like a body of two halves which doesn’t really fit in with CRPS, I was still very much of the opinion this was Coccyx-Axis related and suggested she see a Bowen Therapist, as I felt with the penetrating sit bone pain that a Bowen Pelvic Procedure graduating to Coccyx, TMJ procedures and the Psoas would be beneficial in trying to release the taught right illac fossa against the flaccid left fossa to initiate structural realignment from the neck downwards. It was when Mrs M told me she had had major Orthodontic work as a teenager and recently a repeat of that treatment as the teeth had moved, that that was the key to the Axis-Coccyx relationship married in with Psoas disharmony and abdominal destabilisation after surgery.
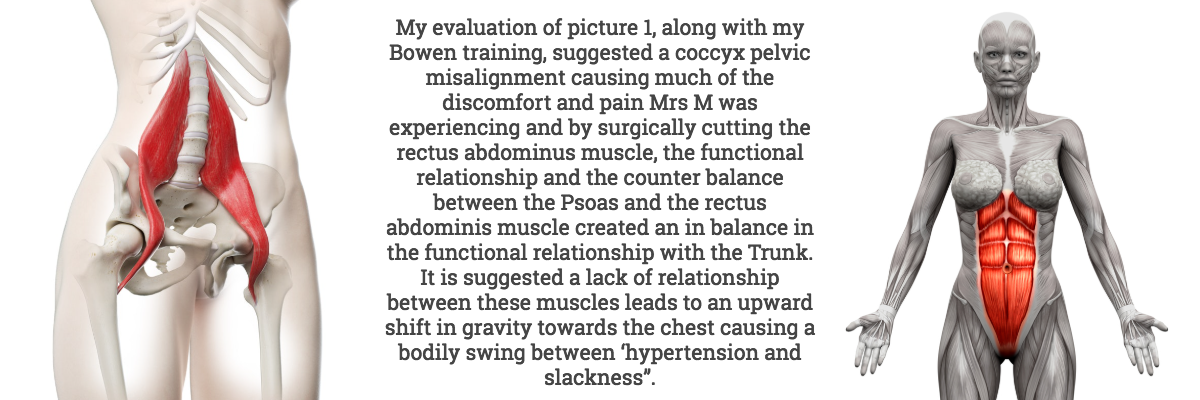
The Psoas is a flexor muscle and contracts whenever the fear reflex fires. I quote from The Psoas Book by Liz Koch, (“When the reflex fires repeatedly, with little recovery time and/or no ability to complete the cycle by fleeing or fighting, a conditioned response occurs that prepares the body for the next attack by maintaining a state of tension. Because the organism no longer has the opportunity to return to a normal state of functioning and nourish itself, the level of tension accumulates. The tension is experienced as anxiety.”)
This might explain why there has been such a catastrophic muscular skeletal alteration due to preoperative and operative heightened anxiety regarding the procedure and by the cutting of the rectus abdominals, which destabilised the trunk functionality from which the body has been unable to readjust and recover.

Picture 4. Less upward pull and scar continuing to fade.

Picture 5. 24.05.2021 The scar is much more midline with little deviation upwards on the right. Right iliac fossa still under some strain.
Practitioner’s Conclusion:

It is deeply regrettable for Mrs M and her family that she has been unable on either birthing occasion to experience a beautifully unique bonding at the moment of birth and ongoing motherhood. In my opinion Mrs M’s scenario is shocking and beyond alarming that the multitude of professional avenues from which help and support was sought failed in all aspects of care and concern, whereby at great personal cost Mrs M has endeavoured to seek answers for herself where in the main they too failed.
DEEP OSCILLATION and the MAGCELL were loaned for three months (two months of which Mrs M was not charged) and in that time they have worked a certain magic. With telephone guidance, the scar is calm and fading, it is a lot less lumpy with a slight lumpiness only to the right side, it should respond to the laser over time. I hope between Bowen Therapy and Postural Rehabilitation Physiotherapy that Mrs M can, after twelve months of clinical failure, regain functional equilateral balance.
I was shown a photograph of a scar, I attained a full medical history over many years, so I could clinically jigsaw together reasons why, as this SCAR runs deep.
Christine Talbot
SRN BLS MLD UK, Vodder, Leduc, LTA Fill & Flush, Casley Smith MLD DLT Practitioner and Lymphoedema Bowen Practitioners. BA Member.
Stoborough Meadow
Wareham Dorset
BH20 5HR
Telephone 01929 556560
Mobile 07881 598 937
Treatment Protocol

In contrast to externally applied, mechanical forms of therapy, (e.g. vibration), the therapy effect of DEEP OSCILLATION® takes place in the tissue itself and works through the entire depth of the tissue layers (skin, connective tissue, subcutaneous fat, muscles, blood and lymph vessels)
DEEP OSCILLATION® helps in speeding up and improving wound healing processes. Through the oedema-reducing and anti inflammatory effect, the local metabolic elimination and alimentation is improved in all tissue layers, whereby tissue regeneration and wound closure are encouraged on many levels. This is documented by the significant improvement in planimetric and biochemical parameters of the wound healing.
Magcell Information
Magcell Microcirc is a hand held device, based on pulsed electromagnetic field therapy (PEMF) which permeates a 3-5 cm depth and is proven to encourage and increase blood flow to the area(Funk et al, 2014):
“MAGCELL® MICROCIRC significantly increases micro-circulation (p < 0,001) while nitric oxide (NO) has a blood vessel dilatory effect. The application of the rotating MagCell-SR to the HUVEC cultures leads to a rapid onset and a significant increase of Nitric Oxide (NO) release after 15 minutes. Thus, frequencies between 4 and 12 Hz supplied by the device improve microcirculation significantly. Therefore, this device can be used in all clinical situations where an improvement of the microcirculation is useful like in chronic wound healing deficits.”
Low level laser therapy (LLLT) Information
"Low level laser therapy (LLLT) is the use of low energy laser light in injuries and wounds in order to improve wound healing, reduce inflammation and alleviate pain. The laser light is monochromatic, coherent and in the red or near infrared spectrum (600 nm – 1000 nm). It is applied at low power density (1 mW to 500 mW/cm2) (“low energy laser”).
In contrast to other medical laser applications LLLT is not a thermal method (i.e. surgical lasers), but produces photochemical effects in the tissue in a similar way to photosynthesis in plants.LLLT is simple to use, effective and cost-efficient and free of side effects. Treatment takes a few minutes and depending on the indication is repeated at longer or shorter intervals and in accordance with healing success.The success of LLLT is based on the following general action principles: tissue regeneration, inhibition of inflammation, alleviation of pain, improvement in circulation, reduction in swelling"Low-Level-Laser-Therapy (LLLT) in Chronic Wounds - Ludwig-Maximilian University Munich, Germany
Magcell® References
Hitrov N.A., Portnov V.V. (2008): MAGCELL® ARTHRO in der Behandlung von Arthrose im Kniegelenk. Die Naturheilkunde 3, 25-27. - English translation (Hitrov N.A., Portnov V.V. (2008): MAGCELL® ARTHRO in the treatment of osteoarthritis of the knee joint. Naturopathy 3, 25-27.)
Reimschüssel A., Bodenburg P. (2009): Niederfrequente elektromagnetische Felder. Erfolgreich in der Therapie der Myoarthritis des Kiefergelenkes. Die Naturheilkunde 5, 28. - English translation: Reimschüssel A., Bodenburg P. (2009): Low-frequency electromagnetic fields. Successful in the therapy of myoarthritis of the temporomandibular joint. Naturopathy 5, 28.
Laser References
Mosca, R. C., et al. (2019). "Photobiomodulation Therapy for Wound Care: A Potent, Noninvasive, Photoceutical Approach."Adv Skin Wound Care32(4): 157-167.
Machado, R. S., et al. (2017). "Low-level laser therapy in the treatment of pressure ulcers: systematic review."Lasers Med Sci32(4): 937-944.
Tchanque-Fossuo, C. N., et al. (2016). "A systematic review of low-level light therapy for treatment of diabetic foot ulcer."Wound Repair Regen24(2): 418-426.
Kuffler, D. P. (2016). "Photobiomodulation in promoting wound healing: a review."Regen Med 11(1): 107-122.
DEEP OSCILLATION References
